Many South Vietnamese sought new identities as they resettled in locations such as California, Texas, Washington State, Louisiana, and the DC metro area including Maryland and northern Virginia. Perhaps surprisingly, Tennessee also became home to generations of Vietnamese refugees and immigrants with intense transnational migration histories. One family’s story is that of my own, whose refugee experience does not follow the typical timeline of helicopter escapees and boat people. Rather, as Humanitarian Operation arrivals, my family’s history offers an illuminating narrative.1This essay draws upon excerpts from an oral history conducted by the author with Đỗ Phương Anh Linh in November 2020, as well as stories from March 2025 told by his younger sister, Đỗ Phương Anh Thư.
My grandfather, Đỗ Phương Anh, was born on July 3, 1935, in the Quảng Bình province of Central Việt Nam during the French Colonial period. In the late fifties and early sixties, Phương Anh was required to complete mandatory military service for young men in their twenties. A former teacher of Vietnamese literature and theology, he paused his teaching career in 1965 at Trường Trung Học Võ Tánh located in Nha Trang to serve as a lieutenant in the Army of the Republic of Việt Nam (Lục Quân Việt Nam Cộng Hòa), more familiarly known as the South Vietnamese Army. South Việt Nam’s government facilitated mass military mobilization in response to intense war escalation and the deployment of US combat troops. This meant my grandfather would leave his academic job to travel with his family to the provincial city of Sa Đéc. There, he was the military’s paymaster, responsible for distributing wages to the soldiers in the South Vietnamese Army, and was also a logistics officer, managing the local squad’s resources and supplies. He completed his assignment in 1970 and was allowed to return to his teaching position in Nha Trang.
As combat intensified, North Vietnamese forces encroached into South Việt Nam, forcing Phương Anh and his family to relocate to Sài Gòn in April 1975. During the following months, the collapse of the South Vietnamese government led to the detainment of former military personnel and civil servants. Upon his return to Nha Trang in May 1975, my grandfather was confronted by communist officials, arrested, and sent to a re-education camp. Too traumatic and horrific for him to recount, my grandfather’s stories and experiences in those camps are lost to time. Yet, the terrors he saw there would manifest perniciously. Years later, when family members brought up plans to return and visit Việt Nam, in total outrage, my grandfather exclaimed that he would never return to a country where he had experienced such atrocities.
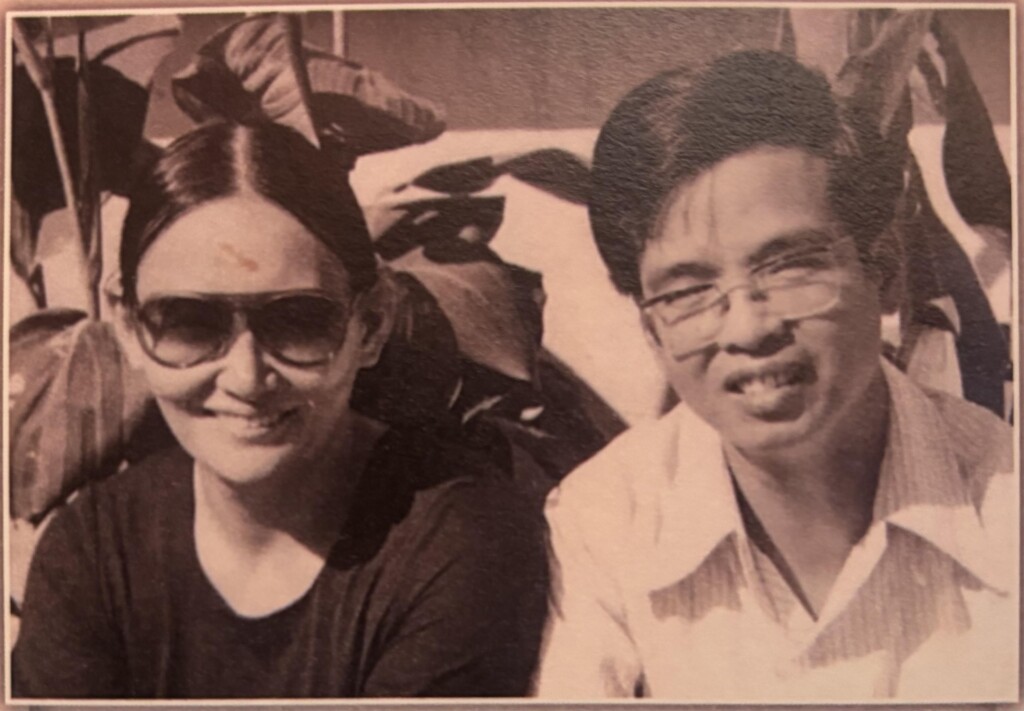
Upon his release in 1982, marking seven years of incarceration, my grandfather faced eviction from his family home in Sài Gòn, forcing him, my father, his siblings, and my grandmother, Lê Thị Kim Hoa, to relocate to government-owned housing. A family of eight, they were crowded into a small, worn-out city property that had no furnishings and limited access to electricity. My father, Đỗ Phương Anh Linh, was born on August 6, 1964, in the city of Nha Trang of southern Việt Nam. Being the oldest son meant he would bear too soon the burden of standing in as the man of the house because of my grandfather’s incarceration. While Phương Anh was in the re-education camp, my grandmother and my father were the only two family members old enough to find jobs. However, neither of them could find decent-paying work in densely-populated Sài Gòn, especially while it was undergoing systematic economic changes as well as recovering from a disastrous war. Circumstances became dire as my father’s family grappled with extreme poverty and starvation. Yearning for new beginnings and exhausted from the suffering and hardship in their homeland, my father’s family decided that they needed to flee to the United States.
At their first getaway attempt, my grandfather and father, together with fifty-three other people, sought to escape Việt Nam by a fishing boat. After seven days of traveling on the South China Sea, commonly known as the East Sea or Biển Đông, a storm caused the boat to malfunction and forced a landing on nearby Côn Sơn island, once a part of French Indochina, but now claimed by the Vietnamese government. Everyone aboard was detained in the island’s prison. My father, age sixteen, was sentenced to one year of jail; my grandfather faced three years. Like many other prisons and detention camps in Việt Nam, conditions were horrible because of food scarcity, compact and crowded living facilities, forced intense physical labor, and a lack of sanitation.
Following my father’s release from the island prison in 1983, he returned to his family in Sài Gòn for a few days before attempting again to escape by boat. This time he travelled without family members to the small city of Cà Mau, where he joined with some seventy other people. Shortly after embarking, the ship’s poor condition caused it to flood. Cast up on a jungle shore, my father tried to find his way back to Sài Gòn, but was stopped by law enforcement at Cà Mau’s city border. He was detained and imprisoned again, this time in Cây Gừa, a local camp.
After months, my father was allowed to return to Sài Gòn and join his family. My grandfather remained imprisoned. The family’s income was left to my grandmother and father. For the following six months, my father’s job was driving people around the city on a cyclo, a three-wheel bicycle taxi. But he, and my grandmother, who sold bowls of sticky rice on the streets, were unable to earn enough to sustain the family and its small children.

After six months in Sài Gòn, my father and his ten-year-old younger brother, Đỗ Phương Anh Tuấn, attempted another escape. With almost no money they made it to Mỹ Tho to board a Mekong River boat that they hoped would take them to the coast. If they could reach the beaches, my father thought he could figure out a way to flee. As the boat drifted downriver, my father realized that the people who sold him the tickets were scammers. The boat was over-crowded and in a dangerously poor condition. The deck began filling with Mekong water. Everyone screamed in panic and fear, forcing the captain to make an emergency landing at a small island. Here, my father and his brother tried to hide in the jungle brush from soldiers and policemen. In the middle of the night, soldiers monitoring the island caught my father’s younger brother, age ten. My father had no choice but to turn himself in. They were sent to a nearby jail. Once the police determined that they were attempting to escape the country, they were sent to another island prison and subjected to forced physical labor. Sentenced for a year and a half, my father was required to harvest rice for ten hours a day in Việt Nam's hot and humid climate. Among other tasks, Anh Tuấn herded ducks into cages for selling in the farmers’ market. Only a child, he was released early. My father continued to be held.
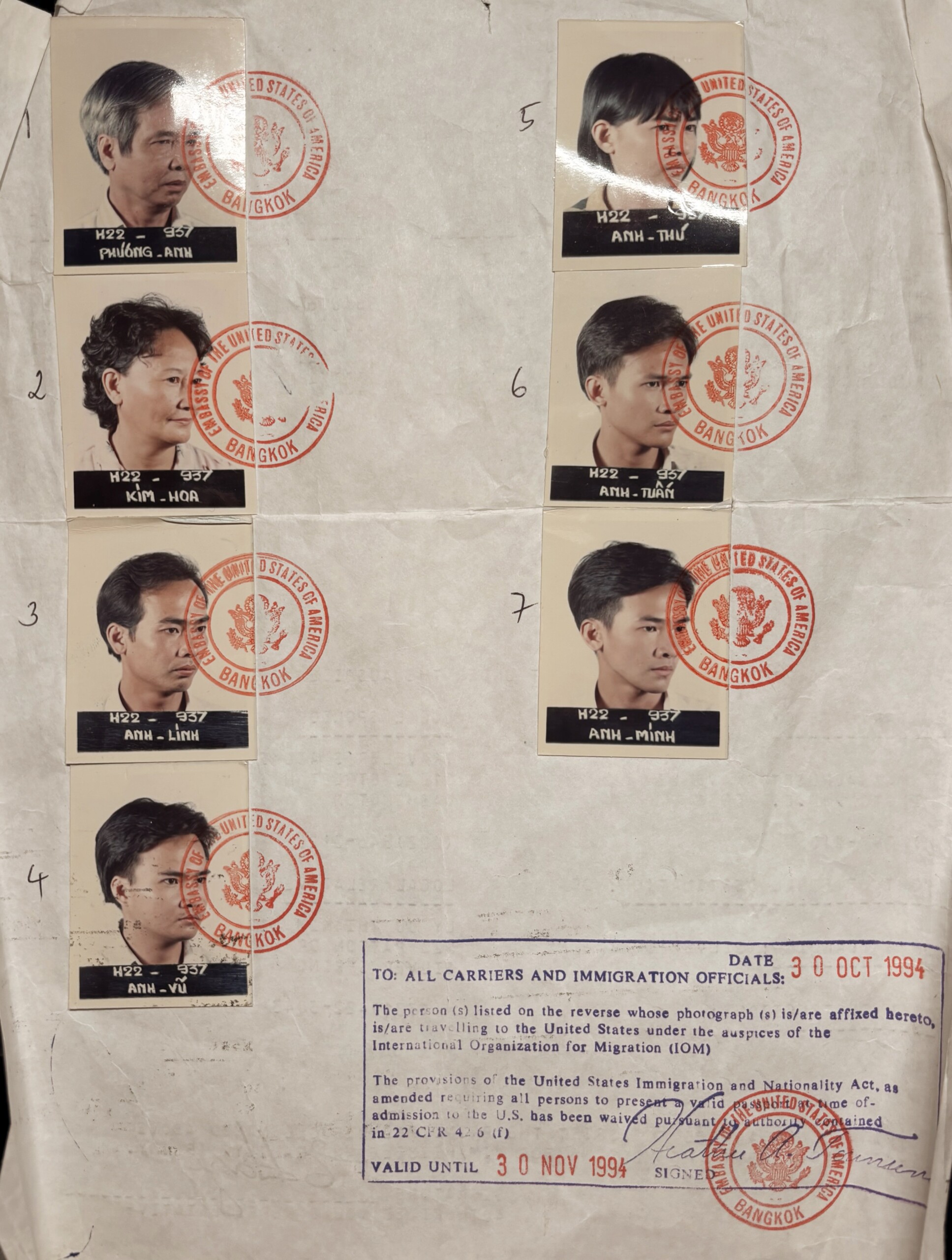
In the early 1990s, the United States began the Humanitarian Operation Program that allowed formerly imprisoned civil servants to seek political asylum. For everyone in my father’s family to be accepted into this program, they had to provide documentation of their time spent within the re-education camps. There was also much paperwork with the US Embassy concerning their applications for a passport and their medical history. After having gone through extended hardship, my father, Đỗ Phương Anh Linh, embarked on this life-changing journey.
In the final weeks of November 1994, my father, his parents, and all five of his siblings flew to Baltimore to reunite with his aunt, Đỗ Thị Kim Liên, and her family. Having lived in Maryland for about twenty years, Liên, and her husband, Lý Văn Đích, arrived in the United States among the initial waves of refugees following the fall of Sài Gòn. At the Baltimore airport, Đích welcomed his relatives and drove them to the family’s residence in Silver Springs. They immediately found work (for around five dollars an hour) at the dollar stores and laundry mats owned by their cousin, Lý Trang.
It had only been three months since my father arrived in Silver Springs when his uncle, Đỗ Quang Châu, phoned and convinced him to move to Tennessee. Châu, more familiarly known as Father Peter, was the former head pastor of St. Martha’s Catholic Church, the first Vietnamese American parish in the Nashville area. After enduring invasive investigations by Việt Nam’s communist government intent on locating the Catholic Church’s financial accounts and stored funds, Father Peter escaped Việt Nam in 1978 by boat and settled in a refugee camp in Thailand. His mother was sponsored in Cookeville, Tennessee, about an hour-and-a-half east of Nashville. To reunite with her, Father Peter flew from Thailand to Tennessee, officially beginning his religious service to a newly emergent Vietnamese Catholic community. Father Peter sought to establish a church where the Vietnamese could worship in their native language. In the nineties, Vietnamese Catholics were constantly relocated and displaced from various churches across the city, with parish staff falsely alleging that the Vietnamese refugees trashed the facilities. Father Peter ultimately led the construction of a new Catholic church in Ashland City that would be the cultural and spiritual hub for local Vietnamese American Catholics for two decades.
When Father Peter contacted my father, he spoke about the Nashville area’s lower cost of living along with its growing job market. My father was dubious, so he went alone to see for himself. He immediately found work at the Sunday School Publishing Board, a Baptist publishing company that created textbooks for churches in middle Tennessee. Father Peter had close connections with the board’s owner, opening the door for many Vietnamese refugees to work there. As Silver Springs, Maryland, became increasingly more crowded with Vietnamese migrants, the ability to find employment had become difficult. The language barrier for Vietnamese refugees meant they were all competing for similar jobs that required minimal English-speaking skills. In Nashville, it was easier to find work, especially physical labor jobs, that required little to no English. My father’s family was convinced that moving to Nashville was their best plan of action, and after six months they joined him there.

At the time, my father was living with his uncle, Đỗ Hữu Đề, who also worked with the Sunday School Publishing Board. Đề was formerly a police chief in the South Vietnamese government. He had previously traveled to the United States, before the war, to study in a police training academy before returning to his family in Việt Nam. Like many other civil servants in the South following the Việt Nam War, Đề was relocated to a harsh and torturous re-education camp. Đề stayed in this camp for ten years, facing starvation and exhaustion from intense physical labor. He was eventually allowed to leave Việt Nam and came to the United States in 1993, a year before my father’s family. Because of his previous studies in the US, Đề was proficient in English, making him a resource and translator among the Vietnamese immigrants. Đề also taught many Vietnamese, including my father and his siblings, how to drive.
My father’s family’s resettlement in Nashville began with a short stay with their Uncle Đề. Father Peter’s advice proved true, demonstrated by the ease with which everyone found employment. Their new jobs varied from working at the Sunday School Publishing Board, a hammer production site, and an electronic assembling company. Their incomes ensured enough financial stability for the family to move out of Đề’s home into a nearby apartment complex. My father and his siblings applied to Nashville State Community College to attain associate degrees. After about two years of clocking into their jobs, keeping up with their coursework, and all the while learning English, the family had saved enough for a major milestone—purchasing a house in West Nashville, where they continue to reside. Finishing their programs at Nashville State, my father and all of his siblings except for his sister transferred to local universities such as Tennessee State and Middle Tennessee State.

By the time most of the family earned degrees (my father’s was in computer science), they had lived in the United States for over five years, the minimum residency to apply for citizenship. They believed this was important, and necessary, because of the legal rights and protections. They saw the right to vote as the most valuable privilege of gaining citizenship, a freedom they were not afforded under Việt Nam’s communist regime. The United Immigration and Naturalization Service (INS) approved their applications and set appointments for their citizenship test – which included a short written section and an oral examination on US history and civics. They all passed on their first tries and were naturalized at a local courthouse in 2000.
Next, my father returned to Việt Nam to marry his long-distance girlfriend, my mother. He helped her get a green card and become a permanent resident. They travelled back to the US in October of 2001 where they were expecting a baby boy. Through countless obstacles and tribulations, my mother and father were finally able to settle and raise a family.
The new life in Tennessee presented challenges and opportunities. The growing Vietnamese population in Nashville found it difficult to attain the varieties of fresh produce, fermented sauces, and particular meat cuts used in their traditional cooking, creating a sense of nostalgia and longing for their beloved dishes.2There are few reliable sources to estimate how many Vietnamese people live in Nashville. As of July 2023, 3.5% of the population in the Nashville-Davidson metropolitan area identifies as Asian (approximately 24,000 people). https://www.census.gov/quickfacts/fact/table/nashvilledavidsonmetropolitangovernmentbalancetennessee/PST045223 Many Asian groceries in Nashville were owned by Lao refugees and immigrants, none that regularly carried the items desired by the Vietnamese. My father and his family took on the challenge of opening a grocery store—now one of the oldest Vietnamese-owned establishments in the area. Along with hoping to fulfill the demand for Vietnamese foods, they wanted to ensure that if any of the siblings were to ever be unemployed, they would have a safety net at the family business. Opening on September 15, 2000, the Đỗ family named their business Bách Thảo Market to represent the diverse selection of fragrant herbs, root vegetables, and leafy greens for sale.

Opening a family business came at a substantial cost. Cleaning out their bank accounts and maxing out credit cards, the Đỗ’s took on a major risk. Driving a box truck fifteen hours each way between Tennessee and Texas, my father was responsible for retrieving two to three pallets of produce and goods that would be sold at Bách Thảo. He carried pillows and blankets with him to create a makeshift truck bed at rest areas on the interstate. My father drove weekly to Texas for seven to eight years until a specialized produce distributor opened in Memphis. In June 2017, Bách Thảo Market was renamed to Little Sài Gòn Market to advertise towards an American clientele, who my family believed would more easily associate Sài Gòn with Vietnamese products versus the less familiar Bách Thảo. Little Sài Gòn Market remains in operation today, owned by Đỗ Phương Anh Thư and Đỗ Phương Anh Minh, the youngest daughter and son among my father’s siblings.
Fifty years after the fall, Vietnamese refugees devastated by war, incarcerated for “re-education,” and displaced to unexpected locations across the United States have created vibrant cultural enclaves. They leave enduring legacies in their new homes, often unknowingly, through simply keeping alive the memories of their motherland. My family’s resilient history, one stream in an intricate Vietnamese American diaspora, suggests the complexity of refugees’ stories and lived experiences—as well as the necessary work of recovering and interpreting this history. 
About the Author
Anhhuy Do is a graduate student in history at Princeton University. Born and raised in Nashville, he is an aspiring scholar of Vietnamese refugees and Asian American history in the US South.
]]>Call for Submissions
Southern Spaces invites scholars, critics, writers, health care providers, public health practitioners, activists, media producers, community organizers, and patients to submit 1,000-word blog posts, as well as longer articles and media productions, that address the continuing public health and political implications of the COVID-19 pandemic. Queries and abstracts are also welcome.
Southern Spaces is an open access, multimedia journal publishing innovative work on regions, places, and cultures of the US South and their global connections. We welcome submissions that creatively examine real and imagined spaces and places through the use of textual, visual media, archival, and ethnographic materials—including artistic expressions.
The COVID-19 series examines relationships between pandemic public health and specific geographies in the US and global South. We encourage interdisciplinary perspectives, critical approaches to space and place, and work that foregrounds the pandemic perspectives and experiences of BIPOC and other marginalized groups.
We are especially interested in individual experiences of Covid that address larger societal questions both in the US and globally, such as:
- How are individual and collective memories shaping and being shaped by conflicting historical narratives of the Covid pandemic?
- How has Covid exacerbated racial, gender, ethnic, and class disparities in healthcare systems and public health infrastructure?
- How did the politicization of Covid impede mobilization for the crisis, affect vaccination strategies and distribution efforts, and/or shape conflicting narratives of the pandemic in the US and globally?
- How has the Covid pandemic differed from previous pandemics such as HIV, polio, the 1918 influenza pandemic, smallpox and yellow fever?
- How is Covid impacting modes of expression for artists and writers?
- How have diverse forms of media carried, shaped, and spread political ideas and religious beliefs related to Covid?
- What are representative symbols and sites of this pandemic (e.g. masks, vaccines, ventilators, Zoom/virtual meetings)?
- How have individuals experienced affective dimensions of the pandemic, including transformative expressions of grief, loss, community, and connection?
- How did the pandemic transform the urban landscape, e.g. occupancy of office buildings; closure of retail stores; restructuring of restaurants and pedestrian spaces?
- How are the over one million lives lost to Covid in the United States being remembered?
How to Submit
Submissions, queries, and abstracts are welcome immediately and will be considered on an ongoing basis. The Covid series is part of Public Health in the US and Global South, edited by Dr. Mary E. Frederickson. Submit all inquiries and materials to Southern Spaces managing editor Mary Ann Robertson at seditor@emory.edu. See the Southern Spaces submissions guidelines for style and formatting. The pieces currently published in the Covid series can be found below under "Similar Publications."
]]>
Southern Spaces: Oh, here's Michelle now. Are you in your RV?
Michelle Fishburne: Yes, I am. As a matter of fact, I'm in the RV at Jordan Lake State Park near Chapel Hill. It's about ten minutes from where I raised the kids. I have a twenty-three-year-old who has struggled with long COVID, but has just graduated from UNC. And then we'll go up to Princeton, New Jersey, where I grew up. I'll be housesitting for two weeks.
Q: We've been intrigued by your book, Who We Are Now. It's an important project. The interviews hit powerfully with regard to the loss and heartbreak from COVID. Sometimes now, in the wake of the pandemic, it's possible to think it wasn't really that bad. Life goes on. But going back to the beginnings and to the following many months as you do, the power of this pandemic can't be avoided.
Let's start with what were you doing when it became evident COVID had arrived and was not going away. What were the early months of COVID in 2020 like for you? When was it evident that COVID was not going to be a two week, stay-home-and-then-go-back-to-life-as-normal situation? And how did you develop the project that ultimately became the book?
Fishburne: I think that moment when I realized this was going to last more than two weeks takes me into early April. In January, I had just gotten back from a wonderful vacation in Grand Cayman and I had told everybody all over holiday break how much I was enjoying my job and that I could just pinch myself. It was just a great job. I was a public relations partnership person for Inmates to Entrepreneurs, some people who really, really needed it. I was working on an event at the US Senate and the House of Representatives. We were talking to John Legend, who was working on something similar, about going into a prison with him.
And then on January 17, an unknown virus attacked my eighth cranial nerve and I lost my hearing in my right ear and my vestibular functioning. I began using a walker and learning to adjust to life without hearing in one ear. In February, I bought a prom dress for my senior in high school. She was very excited about the prom and we were waiting to hear back from colleges.
Then my boss, when he saw COVID coming, he was having some struggles. His doctor said to him, "You know, you can't go anywhere." And so he said to me, "I'm going to have to lay you off because I can't go do any of these things that you are preparing." So I was laid off and I thought, "No big deal. I have a law degree from UVA. I have had an illustrious career. I've done wonderful things. I'll find a job." I wasn't panicked. But I submitted eighty-six customized cover letters between the middle of March and the middle of July, and I had nothing.
The lease on the post-divorce house was coming up on July 31. I knew that on August 1 I would have no house, no spouse, no job, and no kids to take care of. And the big critical moment happened in a Target parking lot on June 15, when I had to decide where to have the movers put my stuff. I thought, "What doesn't make any sense for me is to rent a place because I have no idea where I'm gonna have to go to get a job. I've got the motorhome that I homeschooled my kids in for ten months once. All right, I can move into the motorhome." So I put everything in storage.
And then I thought, "Oh, what will I do? Well, I love the Outer Banks. Take the motorhome to the Outer Banks." But then I thought, "Michelle, you can be in hell while you're in paradise. And if you're waking up every day thinking what's your next job, you're kidding yourself. You need a project."
I could drive out to Yellowstone from North Carolina because I've done it before. Yeah, and then I will cry the entire time I go to national parks because I won't be with my little ones anymore and I'll be all by myself.
Then out of the blue came the idea of Humans of New York. And I thought, "Oh, Brandon Stanton interviewed thousands of people in New York, took their photo, got a little snippet of their story, put it on social media." I could do the same thing. I could do Americans of the pandemic. Who We Are Now—that was the name right from the beginning.
I know that when you focus on other people, it's easier not to be afraid. I also know now from somebody I met during the interviews that action is the antidote to fear.
Getting in the motorhome and doing a fast run helped with my fear. And focusing on other people helped with a different kind of fear. But I was also very naive. What made me think I could go out in the middle of the pandemic and find strangers to talk with?
Q: Your project started off the way interviews work. One person leads to another. But you say that your fear did not seem to have been pandemic related. We're wondering, weren't you concerned about catching the virus?
Fishburne: I wasn't. Once again, naivete really helped. I thought, "I'll just wear my mask and I'll be smart. I mean, I could be smart in Chapel Hill. Why can't I be smart in Saint Louis or New Mexico?" But what I found when I got out into parts of the country that were sparsely populated, I started to reconsider what critical thinking meant.
I did take some risks. I'd think, "Okay, this building is big enough and it's just me and this person. They're way over there and I'm way over here." Because if somebody is going to tell you a story, and they've just met you, and it's about their lives, especially since I only ask one question, what I really needed was for somebody to keep going and going, going and going, right in my face. Inviting them to continue and showing interest. The mouth is really important to that. As much as I tried to use just part of my face and some body language, there were times when I needed to take off the mask.
Q: That makes perfect sense. So you talk about how this book got started, but then you traveled a long road. How did you have the momentum to sustain the project?
Fishburne: It became something unto itself. I'm just a project person and I got in the groove. What sustained me was how surprised I was every single time I got to listen to somebody else. I mean, there were genuine moments of surprise in every single interview. For example, when I talked with Anne, who's the wedding planner in LA, I had in my mind all these questions I was going to ask her because I was interested in how weddings had changed. But when I asked her the one question, she went off in a completely different direction that surprised me.
I think the excitement of knowing I was going to hear somebody else's story is what sustained me.
Q: Who was most helpful in encouraging and supporting you?
Fishburne: My mother, who is now eighty-five, was my sounding board and supporter. She also is an editor. I would send her transcripts of the interviews. I would think, "Well, this person's got different parts of their story in different places in this transcript." So I would move it around then send it back to the person and ask, "Is this what you said?" Or they'd say, "Yes, that's pretty much what I said. Or, "I said 'like' too many times. Can you take that out?"
My mom has a PhD in sociology from NYU. I grew up knowing about qualitative and quantitative research. Knowing how you ask the question is so important. We talked about the question a lot. And I needed to have a grid, a mosaic, to do a representation of the US as best I could. We talked about that, too.
Q: How did you organize your project? And, to get a sense of the scale and the scope of all the interviews you did, how much is included? How much is left out? How did you edit?
Fishburne: I was conscious of what was going on geographically. Age, race, gender, class, they're all in the mosaic. Urban, suburban and rural. Religion of different kinds. There's New York City and there's Jackson, Mississippi. I used a reverse order of population of the top fifty cities to make sure that I got different types of urban places in different parts of the country.
One area I leaned into heavily was the performing arts because they rely on a live audience. And other vocations that really had a hard time. I overloaded those a bit because they were compelling.
I interviewed about three hundred people, but only a hundred are in the book. There are more on the website and there are more that never made their way into a story. One of the peer reviewers called the book "elegiac," not a word I had anticipated. He had seen the book without any photos. Originally the contract was for forty photos, but one hundred people. And I thought, "I don't know how I'm going to choose which forty people." This was December 2021. My editor at UNC, Lucas Church, said, "Maybe we shouldn't have photos in the book. Then it would be elegiac." So the book went without the photos; the way it's set up, it kind of tumbles.
In order to get that tumble feel, some of the stories had to be very short. For example, I spent two hours with Luke and Rodney and only used Luke's story about how he got more grief for wearing a mask than holding the hand of his partner. Lucas said the stories need to be between 250 words and about 1,200. The average interview was probably thirty-five or forty minutes. If the average story length is six-hundred words, which takes about three to five minutes to say out loud, the book has about five hundred minutes of material. And I recorded three-hundred times thirty minutes. A lot was left out.
When Who We Are Now was published—I'm just going to say the truth—it did not do very well. We think what happened is that it arrived during COVID exhaustion. Yeah. More recently, the couple of book clubs that have used it have really delighted in it because it helped them reframe what the pandemic was. I know that however-many-years hence everything that I gathered is going to have more value than it has today. I think in seven years, when I'm sixty-seven, I'm going to be a very popular lady at the ten-year anniversary.
Q: As a historical read as compared with a contemporary read, I think you may not have to wait that long.
Fishburne: Sometimes when I pick it up and I read it—like I just opened up to Tina, the grief counselor—it washes over me. It all just comes back and you think, "Oh, yes, we had to go through that. How do you grieve when you can't have the formal process?"
And then when I was re-reading Tina's story, Melissa's story in Corinth, Mississippi came flooding back. Her mom had died during COVID. And Melissa said to me, "I've always thought it odd when a family member passes and you go back to the home and you have the whole spread of food that people bring. I never understood the importance of it until now. Because now when I walk down the street, it can be a beautiful day, months and months after my mom has passed and I'm having a good day and somebody who hasn't seen me since my mom passed will say, 'Melissa, I am so sorry about your mom.' I didn't get the kind of closure you get with everyone there eating food, drinking, talking."
And in a way that's how it was with COVID itself. It came, peaked, and petered out, but we never had the "end," even though the federal emergency was over. But it's not the end. Especially for people with long COVID.
Q: You mention that Who We Are Now came out around the time of COVID fatigue. But how did these oral histories affect you? Did you compartmentalize them as research?
Fishburne: I didn't see the project as research. It was just my life. Even now, when people talk about the pandemic, most people talk about it in ways that are very foreign to me. And the way I talk about it is very foreign to most people. Before I got in the motorhome and drove around the country, I thought I knew the pandemic experience, but that was based on my own lived experience. When I left here in September 2020, I expected to find desolation, depression, and division. I expected it to be very, very negative. What really surprised me was the human tenacity. The pluck. And that's the word that I use now a lot, pluck, which is spirited and determined.
In doing the interviews, I settled on asking only one question: What was your 2020 supposed to be like and what did it end up being? And people could talk about what they wanted to. They talked about what really mattered to them, what really defined this period of time, and what made it very difficult, or challenging, or surprising.
People who were out in areas that are sparsely populated would say, "Oh, I just went on the same way." But I know having been there, that every person was changed during the pandemic. More than normally every person genuinely thought about other people and what they were going through. And then there were people who were not given anywhere near the support they needed.


Q: And what do you say now, with a bit of distance, in terms of the perspective that you have?
Fishburne: My mom keeps telling me that I'm a sociologist and I keep pushing back and saying, no, I'm a collector of stories because a sociologist goes back and looks writ large. And I don't feel qualified to do that. I centered the project on individuals and offered up each story.
Many people had very difficult experiences of having to go in and try to do their jobs under incredibly hard circumstances. Often, they didn't have the equipment, didn't have the guidance, didn't have the support. They were watching people die or people turned people away. They couldn't do the jobs that they had trained to do. Then people would come in and reject what they were trying to do or tell them they were wrong. That was head spinning. Or to walk into a store and nobody would have masks on because it was a state where you didn't need to have a mask. It was like a horror movie. They'd think, "Which one of you am I going to see next week?" A lot of the people that I talked with in the healthcare field felt like they went through a trauma.
I thought about various groups of people who were struggling. For instance, I talked with Emma, a director of a migrant farmworker nonprofit. She told me about how really nobody cared to protect migrant farmworkers and about one man who died alone in a motel room. That never should happen. In Birmingham, I interviewed Anne, who was running a homeless shelter. She said it got to a moment when she had to ask whether people were safer inside the building or outside.
I had just started eastward in Texas when Governor Abbott announced that you didn't need to wear a mask anymore. I'm like, "What the heck, Texas is a long state to have to go through no matter which way you do it, right up or down or sideways." I was going west to east and had to be in the state for four more days. It became very uncomfortable. I am a political animal so it was really hard for me to not lean into that. But I became so fascinated with each individual. And I thought, "We are all in this together."
But let's take Fox News, on cable all over America right now. And I was really angry at a big part of the country. I'm like, how can you think that way? How can you think that way? It's Fox News. People have had it in their homes for so long. Fox was pitting us against each other, making people angrier and angrier. Some really ugly parts of us came out. But when you actually get in and talk to people, that's not who they want to be. That's not what they want to be thinking about it.
The false narrative that COVID was not as serious as it indeed was really impacted our healthcare workers and public health officials. I interviewed people who had significant responsibilities, including top public health officials in major metropolitan areas, and they stepped away or are in therapy. And some decided not to deal with it affirmatively. One doctor I spoke with recently said, "I can't talk about it." She started the dialogue and then she said, "I can't. I've just put this away in a compartment. I just can't touch it. I just can't do it." But then, there was a nurse who cried at the end of the interview and said, "Oh my gosh, I just really needed to talk about that."
I saw and heard America in these different ways. People trying to get through. It was such an odd time. The challenges we faced were very unusual.
Luke, South Carolina
Mask Wearer—November 2020
We have felt more discriminated against for wearing masks than being gay. And that's crazy. In the United States of America, we are getting more nasty comments said to us in a grocery store, on the street, for the fact that we have a mask on than the fact that we're holding hands as two men. That's just hilariously tragic. Like, that's where we're at? You're really going to be angry that I have a mask on? So no shame or foul to people who don't want to wear a mask—just don't call me a sheep because I have a mask. That literally happened to me at the gas pump this week.
Valerie, North Carolina
State Senator—December 2020

On March 3, I was attending a conference in Charlotte, and I got a text message from Health and Human Services. It was, to put it mildly, surprising to get a text from DHHS out of the blue. They were alerting me that the first confirmed cases of coronavirus in the state of North Carolina were in my district. Two residents of Chatham County who had traveled to Italy had contracted the disease. I knew enough to know that this was huge and that we were on our way into something that was not going to be good. I left Charlotte that day rather than staying over the next night because I knew that if there were two cases, there certainly were more.
When I look back at 2020, coming from that point of entry into where we are now, with massive unemployment because of shutdowns, and then the blowback, the pushback, it has been very, very difficult. We knew the shutdowns were not the best thing for the economy, but having this juxtaposition of the economy versus overall healthy communities was hard. The governor was in a tough position.
And in the midst of all of that, we were waiting on the federal government to bring in aid. When people started to lose their jobs and people's rents and mortgages and car payments went into jeopardy, there was no help. And the state system was not equipped to handle the massive number of unemployment insurance claims. Before COVID, we usually had about 800 or so claims a week. Then all of a sudden, we went from 800 to 1,800 to 300,000.
Our constituents were coming to us saying, "I followed everything you told me, Senator. I filed my unemployment claim and I've waited for three weeks now. When I call, nobody answers the phone. When I go online, I get knocked off. When I do stay online, I keep getting the same thing saying I'm not eligible. I know I'm eligible. I can't pay my rent and my family is going to be out on the street. Can you help me?"
How many of those folks do you think I could help? Very few. And then the small businesses were calling and saying, "Senator, we're not eligible for PPP [Paycheck Protection Program]." Or "Senator, you can only apply through certain banks or lending institutions. I've never done this before. I need technical assistance in applying." Or "Senator, I don't have an established relationship with this bank, so they will not even talk to me. So where's our help?" That's so painful.
And then I got the call that brought everything really close to home. It went like this.
"Hey, Valerie, how are you?"
"I'm good, how are you?"
"Not so good. So-and-so died of COViD."
"No, can't be."
"Yes."
"What happened?"
"Well, you know he had surgery. After the surgery, he was sent to a convalescent center. He contracted COVID there and died in four days."
Two days later, his family asked me if I would eulogize him. The ceremony was on May 2. There was no church service, just a graveside service, because of course we had to be outside. Afterwards, my husband and I just drove around because I just was not ready to go inside. While we were driving, I got a phone call. I had noticed at the funeral that my friend's best friend was not there. Well, so I got the call from another friend who was at the funeral. This is how it went:
"Valerie, I know this is going to upset you, but they found Kenneth dead today."
"What do you mean?"
"That's why he wasn't at the funeral."
He was only two years older than me. Kenneth was the editor and publisher of the Carolina Times newspaper, one of the few Black newspapers in our state. So that's no more. That's the end of an era that started with his grandfather, Louis Austin, way back in 1927.
And so, when I quiet myself, those are the things I most vividly remember.
Frank, Louisiana
COVID-19 Ventilator Patient—January 2021

I was working for a nonprofit organization driving a bus. We would bring older people, people on Medicare, back and forth to doctor appointments, rehab centers. I come home from work, sit down, and watch TV, and all of a sudden, I can't breathe. I called my son and he took me to the hospital. They diagnosed me: "You have COVID." I said, "Man, I ain't got no COVID." The next morning, Dr. M. come and say, "What's the matter?" I'm telling him I come here last night, and the doctor told me I have COVID. I just couldn't breathe. He said, "Are you ready to go home?" I said, "Yeah." So they let me come home. Got home, next day, the same thing. Can't breathe.
They had an ambulance service come get me. They came in here and gave me a breathing treatment and took me to the hospital. And when I got there, on March 24, Dr. M. say he's going to put me in a medically induced coma. I went to sleep on March 24 and when I woke up, it was April 23. I'd been on a ventilator for almost thirty days. The hospital's head of infectious medicine told Dr. M. to unplug me earlier than that, but Dr. M. said, "Man, I'm in the business of saving lives. I'm not going to unplug that man and tell his family he is brain dead, which he's not." When I woke up, I asked my wife when was Easter, and she said, "Boy, Easter been gone." And I say, "Where I been?" And she said, "You been out, asleep." But I didn't remember nothing, and I didn't realize how sick I was until I called my wife and said, "When you come get me?" and she said, "Not right now." I had no idea that I couldn't walk. I had no idea. I couldn't go to the bathroom. I couldn't pull up in the bed. I couldn't use nothing on my body. Hands, legs, feet, nothing. I couldn't do nothing, period, in a vegetative state. I lost the use of everything, man.
They told me they would send me to a rehab center. When I got there, they put me in a room, and the next thing I know, they put me on a second floor by myself and told me that I got COVID again. So I stayed thirty days in there, with everybody masked up, aproned up, gloved up. And they just got me laying there in the bed, can't turn over, can't feed myself, can't do nothing. And nobody could come visit me because I was in isolation. Every time they come in the room, they'd say, "Why are you down in that hole?" "Man, I've been trying to get out of this hole, but I don't have the strength to pull myself up." And then they get mad with you, they'd bring three or four people in and take you out of the hole and then all of a sudden you're back in that hole. Yeah, I mean, I'm laying flat like this for three months. It was supposed to be a rehab center, but they did nothing for me.
I finally got out of there and back to the hospital to do rehab. In two weeks, I was able to stand at the parallel bars and sit in this wheelchair and push up. And then they started walking me, and it was amazing because I hadn't walked in ninety-something days. I got off-balance and never could get the strength. I would walk with a walker and then I would get tired. Like right now, I still get tired fast, I still don't have no balance, still can't taste every now and then, still can't smell every now and then.
I know there's a God 'cause it's a miracle that I am here. The guy's son who does the dialysis tell me, "Mr. Frank, you're a walking miracle." I say, "What are you talking about?" He say, "Frankie, everyone who
was on that floor that had COVID, all of them died but you." And he say, "I know there is a God, you blessed." Then Dr. V., the heart doctor, say, "Man, we really thought you was going to die." Dr. S., "Man, we really thought you was going to die." You know, it's a bad feeling when everybody coming to you, telling you that they really thought you was going to die. And they look at you, "Man, Frank!" and you don't remember. The doctor told me maybe it's good I don't remember. You know? And I'll be asking my wife, "What happened?" And she'll be telling me, and I don't remember. He said, "That's a part of your life that you will never be able to get back." That's fine, I'm here now. I don't wish this on nobody, man.
Emma, Arizona
Migrant Farmworker—February 2021

Our farmworker population start their days at 2:00 a.m., sometimes earlier. Approximately 15,000 to 20,000 of them cross every day, and the lines on the border can be two or three hours long. They leave early so they can make it here in time to get on the bus and be taken to the fields where they harvest the fruits and vegetables that America eats. This area around Yuma is called "America's Salad Bowl." Our organization provides services to our population, including immigration, housing, parenting, chronic disease prevention, and behavioral health. We're always very busy, so when we started hearing the news that this virus was impacting China and how bad it was, we didn't have a lot of time to think about it. We have a small, rural life, so you don't think a lot about whether something international will hit here. You don't think about how interconnected you are in reference to it. Then at the end of January, we had three cases. It was still not a pandemic at that point, and it was just three cases, so we were thinking, Okay, so three cases. We continued business as usual, no additional precautions, just basic hygiene and all that. When the governor issued a shelter-in-place order, we realized this was serious. Shops started closing and people were running around and piling up food and toilet paper.
After our agricultural season ended, a lot of our farmworkers migrated to California, particularly Salinas, San Joaquin, Santa Maria. Then we started hearing about the pandemic hitting them over there, and even some deaths. One man died in a hotel room by himself. The family knew he was very sick. Nobody was visiting him or giving him food or anything, according to the family. The only contact they had was just through the phone, and all of a sudden, he stopped answering. That's how they realized he had died.
During the stay-at-home order, I had a lot of thinking to do about our office here in Yuma. We have thirty employees, and it's important for personal and cultural issues to have direct, one-on-one contact with the individuals we serve. After the two weeks of stay-at-home, we opened the office back up. My husband used to work at the Health Department's emergency preparedness program and helped us understand the precautions we needed to take. We invested a lot of money in plastic safety barriers and hygiene equipment and products, and we had the offices fumigated every two weeks to sanitize them.
Then there was the question of whether to open the doors or lock them and make people knock. But I felt badly for the elderly or the farmworkers who just needed a form to be read or translated or just basic services like that. So I decided that we were going to have to take a risk and open the doors and do whatever we could and pray to God. We were going to face the threats and fight them because we could not be paralyzed; we have to continue serving our population. So we opened the doors. We let people in just two at a time or one at a time to keep as safe an environment for them and for us as possible.
When the agricultural season started back up again in October, the owners of the farms required the workers to wear masks and did temperature checks, but the buses were loaded just the same as before, everyone crowded in. We did two or three campaigns where we went to meet the loading area for the buses at three o'clock in the morning. We provided tote bags with masks, information, gloves, and everything. Our staff was wearing their gowns and PPE, like they were in a hospital. They were there, facing their fears, because what else could we do? One time we gave out about one thousand bags between 3:00 a.m. and 4:30 a.m.
At some point in the pandemic, we were ground zero in the world for the number of cases. The harvest season and the pandemic season collided. Many of the migrants were sick, but they wouldn't say anything. And a lot of them were young, between eighteen and thirty-six, and didn't show symptoms. Migrant workers don't get fringe benefits or sick leave or anything like that, so a lot of them, especially the H-2A temporary workers, didn't want to be quarantined for two or three weeks. So the sick workers wouldn't say anything and then the whole crew would get sick, but they would not say anything. The employers wouldn't say anything either. They wouldn't want the testing to be done for the workers and the workers wouldn't want to be tested, and so there was like this kind of silent agreement. "Don't ask, don't tell, because we need you and you need us." That is what I have been hearing.
Donna, Georgia
Senior Living Community Executive—July 2021
The coronavirus came to our campus on March 13. It was one employee and we sent them home. I then went to my boss, the CEO of our company, and said, "Our best strategy right now is to lock in. We'll ask employees to volunteer to live on campus and we'll reward them. And we will just live on campus with our members. It'll be over in two weeks, four weeks max." He never blinked. He was behind me 100 percent.
We didn't call it "lock out." We "locked in" with our members and we kept the world out. We kept coronavirus out. The gate was literally locked, and the only thing that came in and out of that gate was food deliveries, Amazon packages, and Instacart.
I asked for volunteers from our employee body, and sixty people raised their hands immediately.
They included our director of accounting, our moving coordinator, servers, housekeepers, maintenance, security. I took any volunteer who raised their hand. Ended up being seventy-five. The next step was figuring out where people were going to sleep, how we were going to feed employees, and how we were going to keep the operations of our 500-member community running with a staff of seventy-five instead of 300.
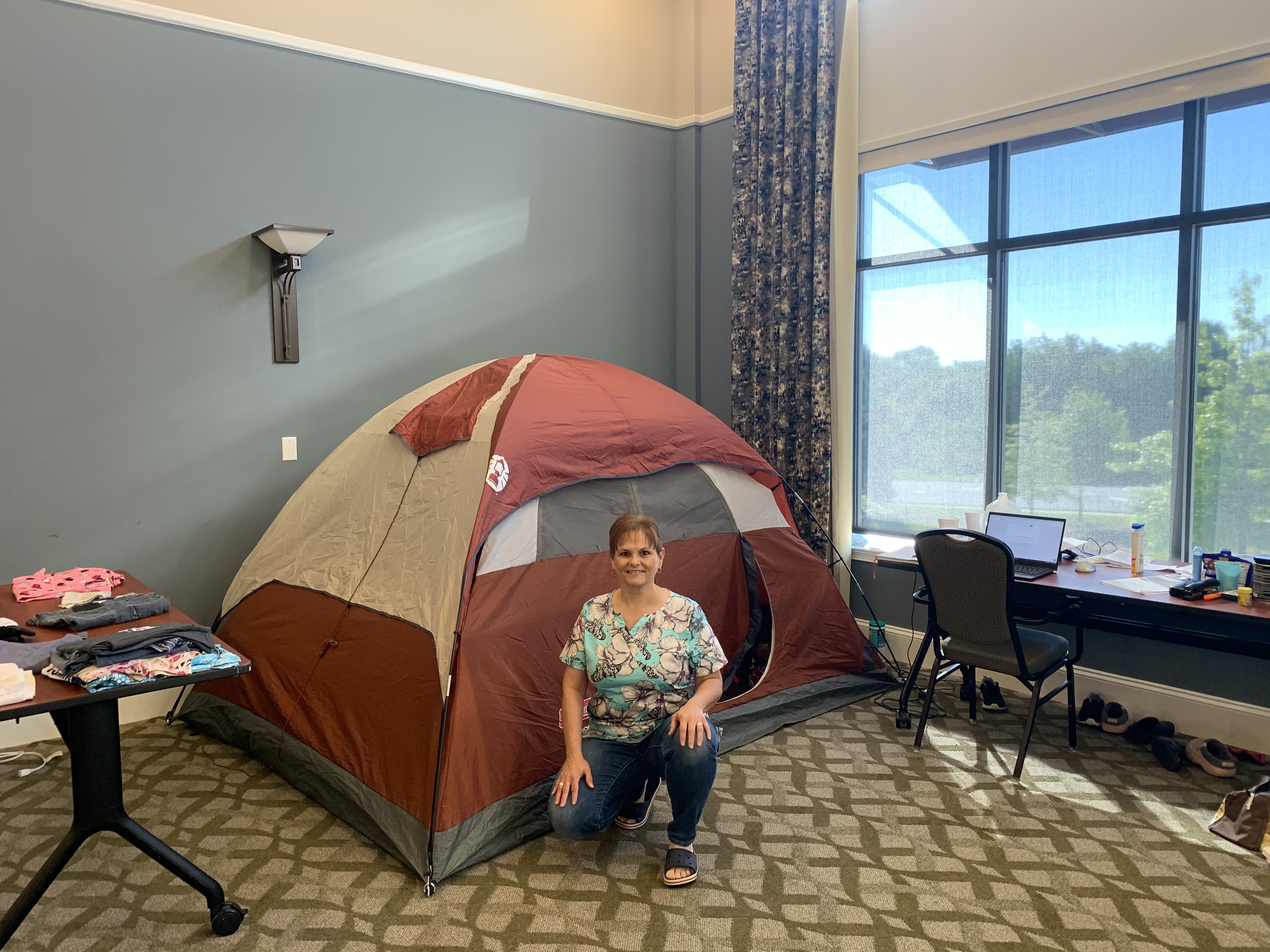
Some of the employees lived in model rooms, some lived in rooms on air mattresses, and some people, like me, lived in our health center, with memory care and skilled nursing. I lived in a tent in the community hall.
We left our titles at the door and we all took on different roles, whatever we needed to do to take care of members. Everybody at mealtime became someone that delivered meals. Everyone became someone who would disinfect our common areas. Everyone became whatever we needed them to be in the moment. I don't even know that some of my employees that I was serving with knew I was the COO. They just knew I was that girl that came and made French toast on Sunday mornings and vacuumed the hallways and helped do laundry. It didn't matter because it was all of us together, fighting a common enemy called COVID.
Each day, I would crawl out of my tent, put on my scrubs and ball cap, and go down to see who needed help with breakfast. I might be feeding a member, I might be cooking in the kitchen, I might be just engaging with members around a game of cards or a board game, or painting nails or giving a haircut. By the time breakfast was over, it was already lunchtime, and we were making sure that everybody was eating and getting their meals. Days were filled with making sure our households were clean, members' rooms were clean, laundry was done for everyone, and everyone received their medications. And spending time together, like sitting outside in the courtyard, soaking up the sun, talking and visiting. We did things to keep people entertained, too, like Zoom karaoke. They got such a hoot out of hearing me sing not well.
We were working twelve, fourteen, sixteen hours a day, doing what was needed and trying to keep everyone's spirits up. It was constant motion. I will admit that sometimes it was nice to retreat to my tent and just turn off the device and just be. I have an Energizer Bunny in my body, so it wasn't so much physically exhausting as much as just mentally exhausting. Retreating to my tent and just being by myself was a relief for me.
Two weeks went by and the coronavirus was a hot-fire mess in Georgia. Then four weeks. I got everyone together and said, "If you need to go home, you can. You did what I asked you to do. You committed for four weeks. But I still need you." That's the hardest thing I've ever had to do as a leader, to say, "You have given me what you promised, but I need more." And every time I did that, they would say, "You can count on me." And that's not about me, it's about what we do here. It's about our mission of loving and serving members. We make a promise to them that they never have to leave, that we will move them through the continuum of care as they progress in age, and that we will always take care of them.
This was a wonderful example of seeing people living our mission in action. It was about living it to the extreme. And it was a beautiful thing. Our employees talk about our members as their second family. We got to live that; we got to see it in action.
Employees made a commitment to leave their own families during this crisis so they could take care of the members of their second family. We have one director of nursing who has six kids, a husband, and her mom who lives with them. She talked to her family, and she said, "I feel like I need to do this." And the family said, "Don't worry about us. You go and do this and we will take care of home." I've got a picture of her standing in a window, looking at her family two stories down, waving up at the window. That's powerful commitment.
Growing up, my father was a soldier who went to Vietnam twice. You know, I was watching my father go off and hoping he would come back. With COVID, we knew we could lose members. If we didn't do extreme things like locking in, we could lose members, and we weren't willing to do that. That's what I learned from my father about mission and commitment.
We locked in for seventy-five days. When we did leave, it was because we had the processes in place, the PPE and testing in place, that we needed to make sure we could take care of our members and employees. But it was so interesting on that last day when everyone was leaving, and their families were meeting them in the parking lot. They all hung out in the parking lot talking, like they didn't quite know how to leave. They were a big family of seventy-three sisters and two brothers, needing to leave each other so they could be with their own families.
I was remembering that the other day when we finally were able to open up to family visits for our members. They had not seen their families in person, to be able to touch and hug each other, for over a year. Our staff, because they remember how emotional they were after the seventy-five days, were standing by the doors, crying, while the families were reuniting in the rooms. They knew.
We all walked away changed. You can't go through something like that and not be changed.
Michael, Texas
Bar Owner—January 2021

Bars are places that people rely on in disasters. We're community hubs, a place where people go to be able to contextualize what's going on. So even people who you might not see in a bar regularly, you'll see them in times of crisis because it's a place to get news, it's a place to get out of your house, and it's a place to be around people in your neighborhood or community and reassure yourself that there's other people like you. That things are going to be okay. This particular disaster, though, was one that featured humans gathering as the disaster.
When we had to shut down, we wanted to find a way to be able to serve our clientele. We have a community of people that rely on us to be there for them for whatever reason they need us.
People don't go to bars because they want to get drunk. You can get drunk anywhere. People go to bars because of the basic human need to connect. Given the way modern society is going, there's more and more separation and less and less connection. As grocery stores have gone from local shops to big-box stores, there isn't anyone there to talk with anymore. Same with coffee shops. And now that everything is automated and delivered, you can sit in your home and order everything you need and have every interaction through a computer.
We were very cognizant of the fact that the people that needed us as bartenders were still going to need us, and probably more because they were stuck at home, so whatever drove them out of their house in the first place, that hadn't gone away. And more than that, their social outlet was gone; their community gathering outlet was gone.
We started livestreaming from the bar. We went on every night for an hour, and we did all kinds of crazy things, like we sang karaoke for them, hosted trivia nights, and sometimes made cocktails. I called it a virtual bar, and we were as interactive as possible with people. Sometimes we had guests come on from other places in the country. We ended up building a really, really strong following. Basically, virtual bar clientele would sit at home and have a beer, or they'd have a drink of their own, and they would come and talk to us and they would watch us do silly stuff. We put out a tip jar that they could put money in for the staff. It was surprisingly powerful.
That lasted for a while until Texas reopened again, very early and very unwisely. At the time, we were getting towards the end of whatever resources we had, so we tried to open as safely as possible. That lasted for a couple of weeks until one of my bartenders got COVID. Then I was furious. Furious that we'd been put in the position of even trying to let people in our place. And so, out of pique, I recorded a video that was basically addressed to Greg Abbott, the governor of Texas. It was a plea from a bar in a pandemic. It ended up getting something like half a million views on social media. What a lot of people didn't realize was that bars were excluded from a lot of the aid being offered to small businesses during the pandemic. We were placed in a position of needing to open as soon as we were allowed to, even if it was unwise.
Pretty much right after my video, Texas closed down again because there was a big spike in cases. It was a big spike at the time, but compared to where we are now, it was nothing. That big spike that closed Texas down in July was a fraction of where we are now.
Mike, Florida
Doctor—January 2021
We have knowledge we learned based on our experiences in past pandemics. Yet, over the last year, we've acted like we learned nothing. That's very disheartening. We have had a lack of direction, and that's been very frustrating. They say that tough times bring out the best in people. It also brings out the worst in people. I have seen benevolence and kindness that was just phenomenal. And I have seen selfishness and self-centeredness that I would never have expected. It's really been an eye-opening experience.
My grandmother used to say, "I've been alive long enough that I have a right to say what I believe, especially if it's true." I'm not even close to her age, but that being said, I also feel that I've been around long enough, and especially around the medical field long enough, more than thirty-five years, that I can be open and honest.
Over the last year, I've become extremely disappointed with people, from leadership all the way down. I've seen political leaders come out and say, "The doctors and the medical experts say this, but I'm going to do what I want to do." And they're supposed to be our leaders. When people say, "I'm not going to follow guidelines because it's an infringement on my rights," I want to ask, "At what point does it become not all about you but all about everybody else and all about society?" Rather than people uniting with a focused approach, which would have led to a lot less suffering and death for many people, many leaders took such a selfish and self-centered approach that it made a bad situation terrible.
And I'll be honest, I would never have foreseen this happening. Previously, I thought that if we had a worldwide pandemic and we knew it and we saw it daily, that we would take the right approach, follow the high road, a consistent approach. We have done none of that.
I work as a hospitalist and do critical care medicine as well as palliative care work. In the Florida panhandle, our COVID hospitalization numbers have been climbing rapidly. From the beginning in March through November, I would have twelve to fifteen patients to work with each shift, with somewhere between two to four COVID patients. Occasionally, I had up to eighteen patients, but that would be a heavy load. On my shift a week and a half ago, I had twenty-six patients, fourteen of which had COVID. COVID-positive patients take about 50 percent more time. So taking care of twenty-six patients was actually like taking care of thirty-nine regular patients. Four of those patients were in the ICU on mechanical ventilators, which takes even more time.
I truly try to provide the best care I can for each patient, but at some point, it's like something's got to give. That is very disheartening to the doctors and nurses and other members of the medical team because we try to give our all, but unfortunately, it doesn't always work. I've taken care of hundreds of patients with this disease, and I've seen dozens and dozens die from it. Yesterday, more than 4,000 people died from COVID nationally. Many of those dying are young, and even more are dying alone.
It's frustrating when the emergency room is packed with COVID patients, the ambulance bays are packed with COVID patients, and we have no ICU beds available for our critically ill patients. I had a patient come in who was not COVID positive, but he was bleeding out from the bottom, terribly, and he had dropped his blood count by two-thirds.
When a COVID patient died, we cleaned the room and then put this guy in there, but he was the only non-COVID patient in the entire ICU. We have other patients coming in who need ICU beds, like patients with acute strokes and severe heart failure. When these patients come in and the hospital tells them, "We don't have any beds, you've got to go to another hospital," that means more time before they're admitted. As they say, every second is brain tissue in a stroke; every second is heart muscle in a heart attack. And we're having to divert these patients because there's no room. And if we can fit them in the hospital but not in the ICU, then they are put on other floors without the equipment and staffing needed to give them the proper care.
I started during the HIV days, so I've been doing this a long time. Now, when I get home after working up to sixteen hours instead of what is supposed to be a twelve-hour shift, I just try to close my eyes, sleep, and let it go. Because I know that I have to go back tomorrow and do it again.
About the Author
Michelle Fishburne is a full-time digital nomad, splitting her time between her 2006 motorhome, Airbnbs, and the occasional housesitting gig.
Public Health in the US and Global South is a collection of interdisciplinary, multimedia publications examining the relationship between public health and specific geographies—both real and imagined—in and across the US and Global South. These essays raise questions about the origin, replication, and entrenchment of health disparities; the ways that race and gender shape and are shaped by health policy; and the inseparable connection between health justice and health advocacy.
Beginning in 2022, the series expands to include 1000-word blog posts, as well as longer commentaries, essays, articles and media productions that address the public health and political implications of the COVID-19 pandemic from multiple perspectives. The series editor for Public Health in the US and Global South is Mary E. Frederickson.
During the night of June 19, 2023, the first federally recognized Juneteenth holiday, an unknown vandal or vandals desecrated by fire a much-beloved child's mid-nineteenth-century headstone in Washington, DC's oldest African American burial ground, the Mount Zion–Female Union Band Society cemetery in Georgetown. For a quarter century, visitors to the grave marker have left objects—dolls, toys, and birthday cards—a practice that harkens to the nineteenth century history of the cemetery. Why has this particular child's memorial become the scene of gift-giving? And why did it become a site of apparent racist attack? Equally puzzling is the identity of the child. The simple, crowned bluestone marker bears the following inscription:
Nannie
Born May 26, 1848
Died May 18, 1856
The identity of "Nannie" has been a mystery for generations. Her short life spanned momentous events in local and national African American history. She was born one month after the ill-fated mass escape of enslaved people on the schooner The Pearl, the largest attempted self-liberation event in antebellum US history. She was two years old in 1850 when the slave trade (although not slavery) within the District of Columbia was banned and the Fugitive Slave Act made life precarious for free people of color within the District. She was four when Uncle Tom's Cabin was published, six when fugitive slave Anthony Burns was arrested in Boston and shipped back to Virginia, enraging abolitionists during the same year the Republican Party was founded. Nannie was seven when open mass violent conflict erupted in Kansas. In the month of her death, the US Supreme Court called for re-argument of Dred Scott v. Sanford, leading to the majority opinion in March 1857, authored by Chief Justice Roger Brooke Taney, holding that persons of African descent "had no rights which the white man was bound to respect."
This essay places Nannie's enigmatic gravesite and headstone in the context of the social, political, and spiritual history of the cemetery. We then propose an identity for the girl commemorated as "Nannie," who died one week shy of her eighth birthday, and consider why her resting place has become a compelling site of emotional connection, commemoration, and resistance. Finally, we speculate as to why persons unknown, on the night of Juneteenth, sought to attack this particular site.
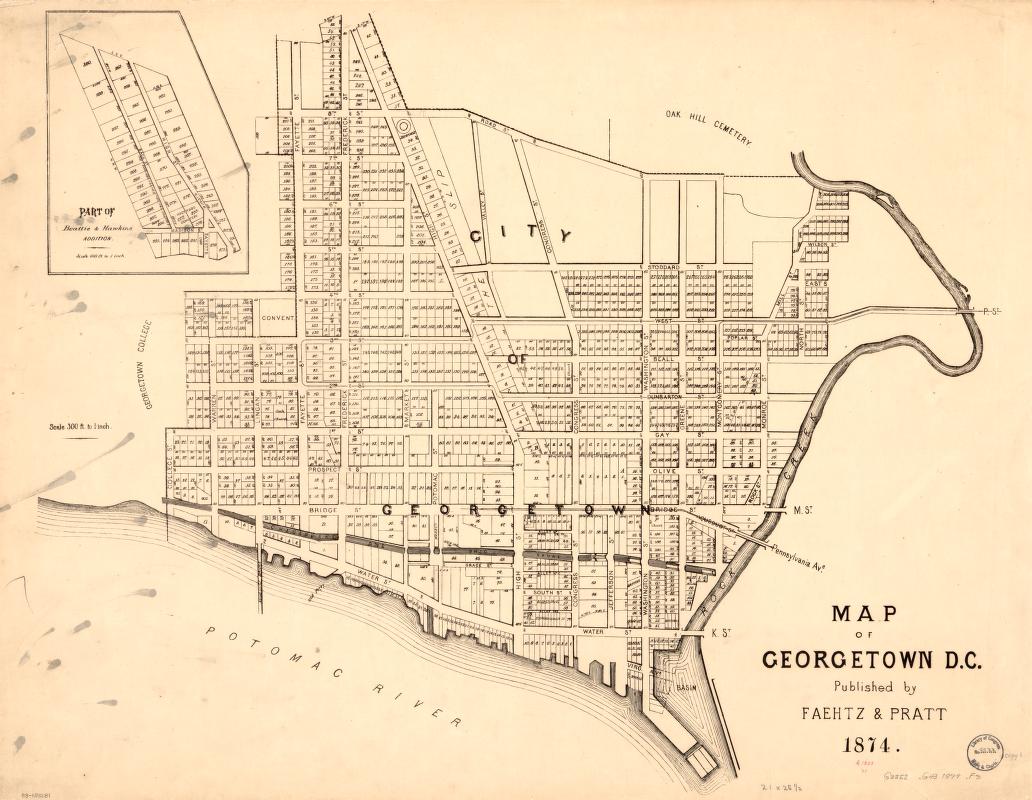
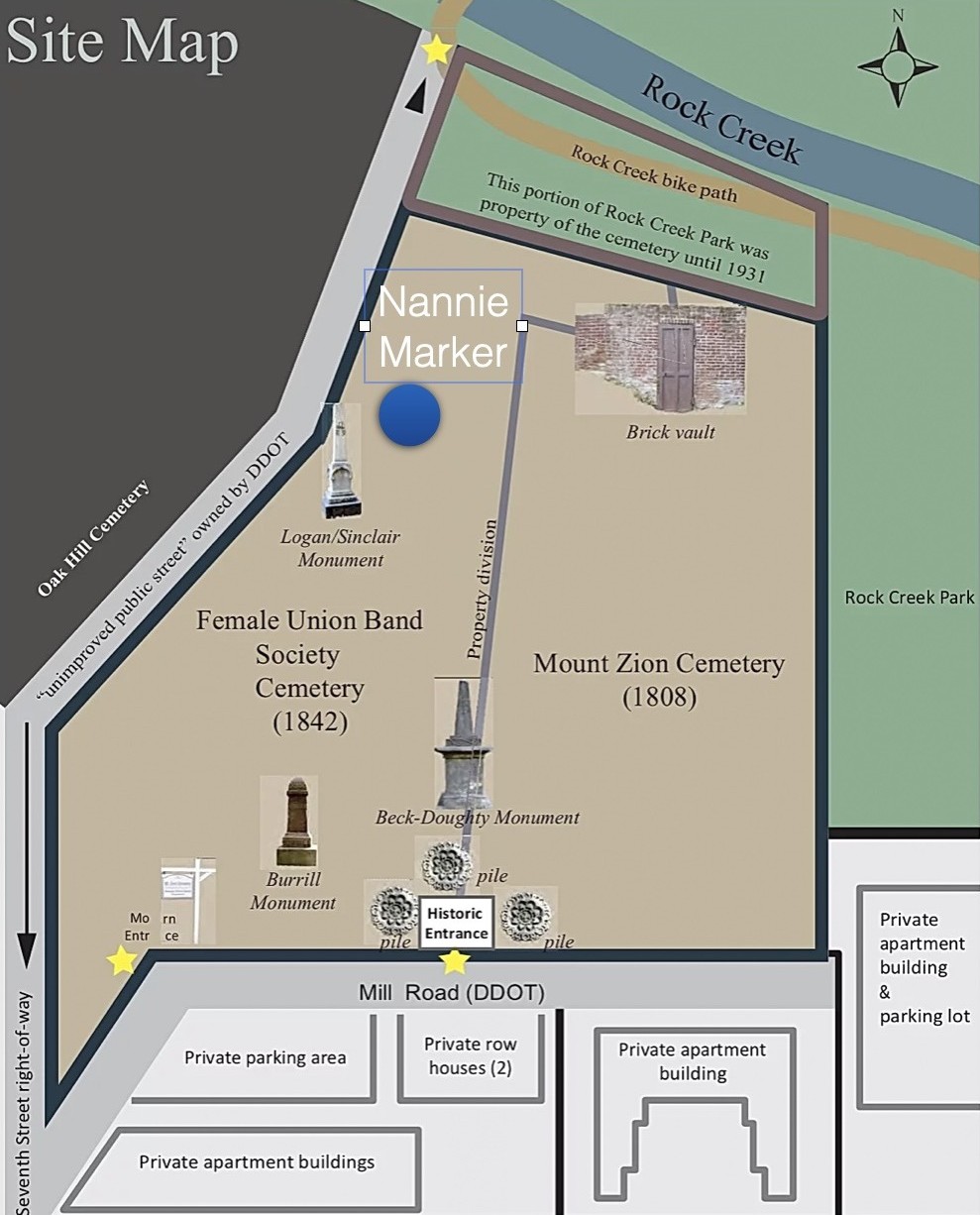
The Mount Zion–Female Union Band Society Cemetery
Many District of Columbia residents have incorrectly assumed that Mount Zion Cemetery is composed of a single burial ground. A three-acre property, it actually consists of two separate but adjacent cemeteries of equal size: the old Methodist Burying Ground (now known as Mount Zion Cemetery), and the Female Union Band Society Cemetery.1Stanton L. Wormley, ed. Mt. Zion Cemetery: Washington, DC, Brief History and Interments, comp. by Paul E. Sluby, Sr. (Washington DC: Columbian Harmony Society, 1984); Paul E. Sluby, Sr., Bury me deep: Burial Places Past and Present in and Nearby Washington, D.C.: A Historical Review and Reference Manual (Temple Hills, MD: P.E. Sluby, 2009). In 1931, the Federal Government took one half acre of the earlier cemetery grounds to create Rock Creek Parkway and an adjacent horse riding trail. The grounds are now under the authority of the National Park Service.
The old Methodist Burying Ground was purchased in 1808 by the Montgomery Street Church in Georgetown, one of the first Methodist churches in the country, founded in 1772 (known today as the Dumbarton United Methodist Church).2The church was formerly located on Twenty-Eighth Street between M and Olive Streets, N.W. (formerly Montgomery Street between Bridge and Olive Streets), approximately one-half mile southwest of the cemetery. At the beginning of the nineteenth century the membership of the Montgomery Street Church was almost 50 percent Black and included free and enslaved congregants. Upset with segregated and racist practices, 125 Black members left Montgomery Street in 1816 and formed the first Black congregation in the District of Columbia, known then as the Meeting House or the Little Ark, and today as Mount Zion United Methodist Church. The two Methodist churches, white and Black, continued to share the Methodist Burying Ground until after the Civil War.3The land was purchased from Thomas Beall, who had inherited extensive property from his grandfather Ninian Beall (1630–1717). In the early nineteenth century, Beall owned about fifteen slaves and many properties in Maryland and the District of Columbia, including the properties now known as Dumbarton House, Beall-Washington House, Conjuror's Disappointment and Rock of Dumbarton. He served in the 1790s as the second Mayor of Georgetown and played an important role in establishing the District of Columbia. On Dumbarton Methodist, see: Jane Donovan, Many Witnesses: A History of Dumbarton United Methodist Church 1772–1990 (Washington, DC: Dumbarton United Methodist Church, 1998); J.W. Cromwell, "The First Negro Churches in the District of Columbia," The Journal of Negro History 7, no. 1 (1922): 64–107; Janet Lee Ricks, "Mt. Zion United Methodist Church Marks 185th Anniversary," Washington History 13, no. 1 (Spring/Summer 2001): 71–73.
Around 1832, a group of free women of color formed a benevolent organization, the Female Union Band Society (FUBS). A decade later and for $250, they engaged Joseph T. Mason—schoolteacher and free man of color—to purchase a plot of land adjacent to the Old Methodist Burying Ground to use as a burial ground for the society's members and their families. Court records indicate the land was acquired from Joseph E. Whitehead of New Orleans. Mason ran a school within the Black church that after 1844 was known as Mount Zion Methodist. If Nannie was a free child of color in the vicinity, Joseph Mason most likely taught her as a pupil.
It is also believed that these burial grounds also served as a refuge on the Underground Railroad. Mount Zion Church and the burial holding vault located on the Mount Zion Cemetery property are said to have opperated as hiding site for escaping "passengers" heading north. Over the first half of the nineteenth century, the numbers of enslaved in the District of Columbia declined. By 1850 (when Nannie was two years old) 3,185 of the 13,746 Black inhabitants are listed as enslaved. In DC, enslaved and free persons often lived, worked, and worshipped together, although their life conditions were often precarious.4Pauline Gaksins Mitchell, The History of Mt. Zion United Methodist Church and Mt. Zion Cemetery, 51 (Washington, DC: Records of the Columbia Historical Society, 1984): 103–18. The History of Mt. Zion United Methodist Church is 51st separately bound book; Stella Mae Richard, "Two Hidden Cemeteries in the Georgetown Section of Washington D.C.," Negro History Bulletin, Washington 32, no. 8 (Nov 1969): 29.
In 1849, Oak Hill Cemetery, reserved for white burials, was established by the financier, philanthropist, and former slaveowner William Wilson Corcoran (1798–1888), later denounced as a Confederate sympathizer, who after the Civil War founded the Corcoran Gallery of Art.5In 1830, Thomas Corcoran, William Wilson Corcoran's father and sometime mayor of Georgetown, owned five enslaved people. The 1840 census indicates that William Wilson Corcoran owned one male enslaved person between the ages of ten and twenty-three and three free women of color, who may have been previously enslaved by him; all resided in his household. In 1845, William Corcoran manumitted the enslaved woman Mary and four of her children. (National Archives and Records Administration, Records of the U.S. Circuit Court for the District of Columbia, Records of Manumission, vol. 3, Record Group 60, Washington, DC; cited in Mark Laurence Goldstein, "Capital and Culture: William Wilson Corcoran and the Making of Nineteenth-Century America" (PhD diss., University of Maryland, 2015), 30–31. This woman may appear in the 1850 census as Mary Degges, born 1819, married to Judson Degges, with children Adelia, born 1834 and Mary, born 1837. Corcoran's "Last Will and Testament," September 6, 1887, provides a stipend of $200 to a woman named Mary Neale, "once owned by me, and long since manumitted." This person may be the Mary Neil who evidently married John Neil in 1875, and may have been born as Mary Degges, daughter of the older Mary Degges. This 22.5 acre cemetery sits adjacent to the Female Union Band Society Cemetery and is separated by a sliver of elevated land, Lyon Mill Road, that served as a path leading to a mill within present-day Rock Creek Park. After Oak Hill opened, whites at the Methodist church gradually abandoned the Methodist Burying Ground and began to disinter their white relatives and re-bury them in Oak Hill and other "white only" cemeteries around the city. Early references to the area that became Mount Zion Cemetery are to the "Methodist Episopal Burial Ground of Georgetown," the "Old Methodist Burial Ground," or the "Colored Methodist Burial Ground."6Richard P. Jackson. The Chronicles of Georgetown DC from 1751 to 1878. (Washington DC: R.O. Pokinhorn, Printer, 1878), 270; Wesley E. Pippenger, District of Columbia Interments (Index to Death), January 1, 1858 to July 31, 1874 (Westminster, MD: Heritage Books, 1999), xix. The land in question is north of Q Street and east of Lyons (Mill) Road (now an extension of 27th street) and Oak Hill Cemetery, extending down hilly slopes to Rock Creek. Over time, the eastern section of this burying ground became known as Mount Zion Cemetery (or Mount Zion East) and the western zone as the Female Union Band Society cemetery. By 1879, white parishioners entirely ceased using the Old Methodist Burying Ground and leased it to Mount Zion Church for ninety-nine years, its name officially changing to "Mount Zion Cemetery."
As racist policies and practices pushed many Black residents out of Georgetown over the next half-century, the cemetery suffered neglect and abandonment. The final burial in Mount Zion took place in the early 1950s. The District's department of health condemned the two cemeteries in 1953, prohibiting future burials. In the 1960s, developers sought to buy the land and disinter the remains in both burial grounds. African American activists, including the Afro-American Bicentennial Corporation (ABC), energetically resisted these plans, and in the mid-1970s secured court and appellate rulings that safeguarded the cemeteries' futures as a memorial park, with disinterments prohibited. As part of planning and restoration, many headstones and markers in both cemeteries were relocated and consolidated in 1975, evidently with the intention of restoring and returning them to their original positions. However, given the fragility of the stone tablets, they were left in place and not returned.7Before the moving of the stones, Mount Zion stones were mapped with a good deal of detail; the Female Union Band Society mapping was, it appears, less thorough. Richards, Two Hidden Cemeteries, 29; Mitchell, The History of Mt. Zion United Methodist, 103–118; Kathleen Menzie Lesko, Valerie Babb, Carroll R. Gibbs, Black Georgetown Remembered: A History of its Black Community from the Founding of "The Town of George" in 1751 (Washington, DC: Georgetown University Press, 2016); Steven J. Richardson, The Burial Grounds of Black Washington: 1880–1919 (Washington: DC: Records of the Columbia Historical Society, 1989), 52: 304–326. Burial Grounds is the 52nd separately bound book.
The cemeteries were added to the National Register of Historic Places in 1975. The joint cemetery is now maintained by the non-profit Black Georgetown Foundation (until recently The Mount Zion–Female Union Band Historic Memorial Park, Inc.) The cemeterties' survival and restoration in the face of powerful white-dominated development interests is celebrated as a miraculous point of deep pride. It is located at the very top of Georgetown, one of the wealthiest and whitest quarters of the city, adjacent to Oak Hill Cemetery, where many of the city's elite white residents have been interred since the mid-nineteenth century. It sits besides Dumbarton House, a structure long associated with prominent white slaveowning families, now the national headquarters of the Colonial Dames of America. It overlooks Rock Creek Park, the greenway that connects the metropolitan area's wealthy northwestern suburbs to the downtown seat of government. The cemetery represents, for many, a defiant unofficial monument to Black struggles for self-determination in a historically Black city undergoing rapid gentrification, still denied statehood and Congressional voting representation.8US District Court Judge Oliver Gasch reversed the order allowing disinterment by developers in order to build condos, stating that such action by the heirs and developers "cannot but offend the sensitivities of civilized people." "Equally important," said the judge, "is the fact that not only would such a degradation be perpetrated against the dead, but in this instance the violation of their graves involves the destruction of a monument to evolving free black culture in the District of Columbia." Female Union Band Ass'n v. Unknown Heirs at Law, 403 F.Supp. 540, 547 D.D.C. 1975.
Gravesite Objects as Memorialization Practices
Since organized efforts began in the 1970s to safeguard and restore Mount Zion, volunteers have often come across bottles, pottery shards, sea shells, and related objects. Frequently dismissed by officials as "debris" or "trash," these objects are interpreted by guardians of the cemetery as traces of much older Black memorialization practices, dating back into the era of enslavement.
Strong evidence for this interpretation is provided by a series of newspaper articles, widely reprinted during August and September 1894, documenting popular memorial practices in Mount Zion cemetery. Local African Americans regularly placed objects associated with the life experiences of the deceased on gravesites, including medicine bottles containing residue of medications taken during final illnesses.9Versions of this story are reprinted in the Gazette (York, Pennsylvania), 10 Aug 1894, 5, The Clarion Ledger (Jackson, Mississippi), September 10, 1894 and many other newspapers in August and September 1894. In the articles, Sexton Henry Bowles (c. 1840–1907) explained that familiar toys and tools encouraged the spirits of the dead to "confine their manifestations to the cemetery," rather than haunting the living. On the grave of a "Mr. Johnsing" (perhaps Henry Johnson, who died in December of 1893) his widow placed a wooden hobby horse, "buried up to its haunches," commemorating the dead man's occupation as an express wagon driver, as well as his beloved horse. Each night, she explained, her late husband's spirit would hitch and unhitch the wooden horse, and thus be distracted from tormenting his surviving kin. The half-burial of the horse evoked the object's transitional status, mediating between the realms of the Living and the Dead.
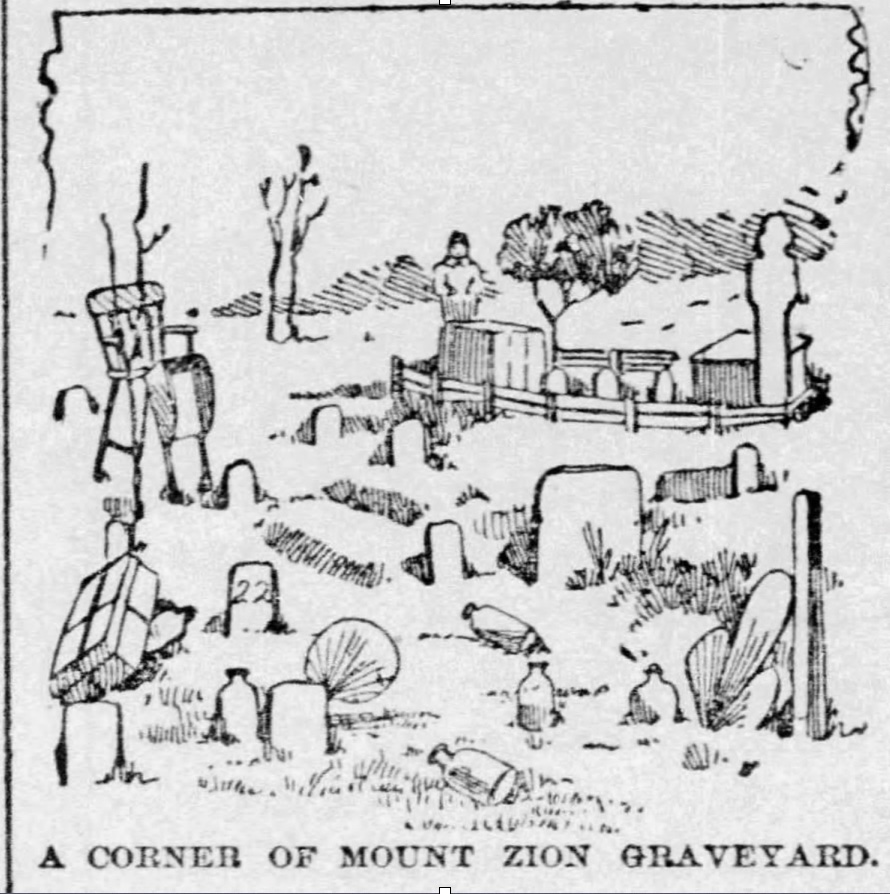
Placed on the grave of a young boy, a high chair and toy wheelbarrow signified objects of importance in his life. A woman named "Lize Lundy," who was fond of wearing a new bonnet to church each Sunday, was honored with her final bonnet and a hand mirror placed on her grave. A particularly complex grave assemblage, perhaps for a military veteran, featured a mound guarded by two large toy soldiers, with smaller soldiers in front of each large soldier; at the mound's center stood three upright bottles. The items may be thought of as "transitional objects," easing the transition from one life stage to another. By repeatedly touching intermediate objects, mourners gradually come to terms with a painful loss and in time relinquish the full burden of their immediate grief.10D.W. Winnicott, Playing and Reality (London: Tavistock Publications, 1971); Melanie Klein, "Mourning and Its Relation to Manic-Depressive States," The International Journal of Psychoanalysis 21 (1940): 125–153; Ellen Schattschneider, "Buy Me a Bride: Death and Exchange in Northern Japanese Bride-Doll Marriage," American Ethnologist 28, no. 4 (2001): 854–880.
These practices are consistent with vernacular African American grave decorations widely documented throughout the Americas, having African antecedents, and transmitted by enslaved and free people across the generations.11Jamieson, Ross W., "Material Culture and Social Death: African-American Burial Practices," Historical Archaeology 29 (1995): 39–58; John Michael Vlach, The Afro-American Tradition in Decorative Arts (Cleveland, OH: Cleveland Museum of Art, 1978). Bottles, shells, pottery and other elements are held to ward off mystical dangers and ease the Dead's transition into the other world and towards ancestral status.12Thompson, Robert Farris, Flash of the Spirit: African & Afro-American Art & Philosophy (New York: Random House, 2010); Vlach, The Afro-American Tradition in Decorative Arts, 142; Savannah Unit Georgia Writers' Project Work Administration, Drums and Shadows: Survival Studies among the Georgia Coastal Negroes (Athens: University of Georgia Press, 1940).
The Nannie Stone in the Modern Era

Public attention to Nannie's gravesite is largely due to the efforts of Omar "Casey" Ibrahim, born around 1936, who during the summer 1997 worked as a volunteer to clear and help restore the cemetery, much of which had been inaccessible due to fallen limbs and extensive weeds and vines. At an October 1997 ceremony, Ibrahim pointed to Nannie's burial site, which was marked only by a fallen-over slab. He urged each person to adopt a gravesite to care for. "I've adopted Nannie . . . I'm going to set her stone up straight and clean all around there. Then I'll put up a little red fence. And then I'll give her a teddy bear and other toys that children like."13Linda Wheeler, "Black Church Honors it Historic Cemetery," Washington Post, October 14, 1997. Mr. Ibrhaim and his daughter continued to place objects at Nannie's memorial for several years. Inspired by this example visitors across the subsequent years have placed objects, including dolls, ribbons, toys, and birthday cards, in front of the Nannie headstone.14Theresa Vargas, "Someone Keeps Leaving Toys and Birthday Cards at a 7-Year-Old's Grave in a Historic Black Cemetery. No One Knows Who," Washington Post, April 17, 2021. The marker has catalyzed speculation and a series of commemorative art works, including by artist Lindsey Brittain Collin, inspired by dolls left at Nannie's graveside.
Nannie's grave marker is currently located within the old "Female Union Band Society" section, at times referred to as "Mount Zion West." The headstone is propped up against a tree. Like many stones in the cemetery it has been moved at least once. Its original location is not marked on the 1970s' survey, but was well within this section—which means that Nannie was almost certainly a child of color who was part of the substantial free Black population residing in Georgetown and other DC neighborhoods. It is possible, however, that she was enslaved for some or all of her short life. Slavery was legal in the District until April 16, 1862, when an act of Congress instituted a compensated emancipation system.15Mary Mitchell, "'I Held George Washington's Horse': Compensated Emancipation in the District of Columbia," Records of the Columbia Historical Society, Washington, DC 63/65 (1963–1965): 221–229; Reidy, Joseph P, "The Winding Path to Freedom under the District of Columbia Emancipation Act of April 16, 1862," Washington History 26, no. 2 (2014): 18–22. The complex relationships between enslaved and free persons of color in the antebellum District of Columbia are examined in Mary Corrigan, "A Social Union of Heart and Effort: the African-American Family in the District of Columbia on the Eve of Emancipation" (PhD diss., University of Maryland, 1996). The broader context of DC emancipation is addressed in Kate Masur, An Example for All the Land: Emancipation and the Struggle Over Equality in Washington, D.C. (Chapel Hill: University of North Carolina Press, 2010).
Considering "Nannie"
Who was Nannie, and why was this striking headstone? The inscription is done professionally and with great care, which suggests that it was paid for by someone of means, or with access to a network of supporters who helped fund the purchase.
Why was only the child's first name used, given that surnames are usually inscribed on Mount Zion–FUBS headstones? Possibly because the child was buried within an extant family plot that was obscured through the relocation of markers in the 1975. Or, if Nannie had been fathered by a prosperous white man with a woman of color, outside of wedlock, the father might have paid for a headstone, but been unwilling to authorize his surname.
The name Nannie, like Anne, is derived from the Hebrew term for favor or grace. Nannie was sometimes a diminutive for Ann, Agnes, Nancy, or other girls' names. "Nannie" was also a girl's name in its own right in the mid-nineteenth century. The 1850 census records about seventeen free women of color named "Nannie" living in the United States. The 1870 census, the first to list all African Americans, lists about two-thousand black women named Nannie. An obelisk to Nannie Diggs, who died October 23, 1923, at age sixty-on, was erected by her daughter Katie Anderson in the same section of the cemetery as the headstone to the mysterious child "Nannie." The records of the Mount Zion–FUBS cemetery list two other Nannies: Nannie Diggs, born 1852 in Virginia, and a Nannie Washington, born 1858, also in Virginia. The most prominent Black Washingtonian bearing the name "Nannie" was the pioneering educator and religious leader, Nannie Helen Burroughs, 1879 –1961, born in Virginia, and a member at 19th Street Baptist. Two months before the death of the young "Nannie" buried in Mount Zion, the Evening Star (DC) reported the death of "Old Aunt Nannie," an enslaved woman at the purported age of 112 years near Powhatan Courthouse, Virginia."16Evening Star (Washington, DC), March 6, 1856, 3.
A Candidate for Nannie: William Teney's Child
Official registers of death were kept in the District of Columbia for Black and white burials from 1855 onwards. However, a register of burials of the Joseph F. Birch Funeral Home, was kept from January 1, 1847 for white and Black burials, and is an invaluable historical resource. Children's deaths were listed by the name of the parent (usually the father) followed by the word "child." The Birch's "Register of Burials, Colored Persons" begins with death #1, January 11, 1847, "Colbert's child," buried in the "Colored Methodist Ground" (the cemetery later known as Mt. Zion). Nineteen pages later, under May 1856, the register lists death #368, "Wm Teney child," as interred in the same Colored Methodist Episcopal Burial Ground. The precise date of death is somewhat ambiguous. The previous line, for death #367, is clearly May 11. Then, for William Teney's child, inverted double commas, indicating ditto, are given for the death date, which would seem to indicate May 11, whereas "our" Nannie, according to her headstone, died one week later on May 18. Nonetheless, other aspects of this child align with our search.17Paul E. Sluby and Stanton L. Wormley, eds., Register of Burials of the Joseph F. Birch Funeral Home, Volume I, (Washington, DC: Columbian Harmony Society, January 1, 1847–April 12, 1864). Also available as FamilySearch microfilm #008135478. Note that a reference to "William Tenney child," is not listed in in Pippenger, District of Columbia Interments.
The most reasonable candidate for William Teney strikes us as a free Black man William Tinny, age twenty or thirty, laborer, born in Maryland, listed with his family in the 1850 census. He is married to Bridget Tinny, born Maryland, age twenty-four, with three children: Sarah Tinny, age seven, born in Maryland c. 1843: Mary Tinny, age five, born in the District of Columbia, c. 1845; Francis Tinny, age three, born in the District of Columbia, c. 1847. Of these three children. Francis, who is born around 1847, is not mentioned in the 1860 census or other subsequent records, and is thus a strong candidate for "our" Nannie. Although Nannie was not a standard nickname for Francis in the period, it seems possible that Nannie was a term of endearment used for her within the family, perhaps rhyming with "Frannie."18Francis's father William appears in a November 15, 1827 District of Columbia manumission record:
"Know all men, by these Presents that I Charles Teney of Washington County in the District of of Columbia for divers good causes and considerations, me thereunto moving [?] and also in further consideration of the sum of one dollar to me in hand paid have released from slavery, liberated and manumitted and set free, and by these present do release from slavery, liberated and manumit and set free my slave woman named Matilda Teney aged about thirty five years, and her three children Anne aged about thirteen years, Andrew aged about three years and William Don Otious aged about 19 months, and able to work and gain a sufficient livelihood and maintenance, which said mentioned slaves were obtained by me as heir at law of my son William Don Otious Teney late of said County deceased, and them the said Matilda and her three children, Ann Andrew and William Don Otious I do declare to be henceforth free, manumitted and discharged from all manner of servitude and service to me and my executors, administrators, or assignees forever. In presence of Lemuel J Middleton and A Balmance."
Two other candidates for "Nannie" are suggested by comparing the 1850 and 1860 censuses: (A) The daughter "Ann" (born about 1848) of freed-people Francis Yates and Caroline (Smith) Yates, who later took the surname Cole, does not appear in the records after 1850. Francis and Caroline married three months before the birth of the "Nannie" memorialized on the headstone. Anna Yates, Black, one year old, died 10 August 1857 and was buried in Ebenezer African Methodist Episcopal burial ground; she may be related, but is clearly a different person; (B) Ann E. Twine, the daughter of coachman David Twine and his wife Caroline Gray Twine, both free persons of color in the District. David Twine was interred in Mount Zion in 1894. A member of Metropolitan A.M.E., David Twine came from a family with long connections to Georgetown and the local Black Methodist community. Both of these girls appear in the 1850 census but are not enumerated in the 1860 census or other records. However, Ann E. Twine may appear in the 1860 census as "Eliza Twine", ten years old, living with an older couple that may be her grandparents. Neither girl is indicated in the DC Register of Burials, so they seem much less likely candidates than the child of William Tenney, who died in May 1856 and who is recorded as interred in the "Colored Methodist Burial Ground."
Francis Tenney (c.1847–c.1856) was born into a free family of color who had been free in the District of Columbia for at least twenty years prior to her birth, and who had struggled intensively to achieve freedom. As noted in the appendices, her family clearly had an extensive network of free kin in the District of Columbia who in 1856 might have pooled resources to enable to purchase and inscription of the well-made headstone.
Desecration
During midday on Monday, June 19, 2023, the first time Juneteenth had been celebrated as a federal holiday, over two-hundred people gathered in Mount Zion-Female Union Bank Society Cemetery to honor the burial ground and the history of African American liberation. The event, organized by the Black Georgetown Foundation, which oversees the two burial grounds, had been widely advertised on social media and radio. Attendees, many of them first-time visitors to the site, were moved by the story of the struggle to preserve and document the cemeteries and the lives of those interred. The event culminated with a gathering in front of Nannie's headstone, where speakers reflected on the enigmas of her life and the history of antebellum Black Georgetown.

During the night of June 19–20, a person or persons unknown set a fire in front of the Nannie headstone, destroying or damaging toys and objects left as offerings during the previous year and leaving dark burn marks on the stone. The attacker was likely aware of the connection felt by thousands of people to Nannie, the preceding day's events, and the fact that in recent years this marker has, more than any other memorial on the grounds, compelled the greatest number of gifts.
The gravestone desecration and the burning of the objects was a form of racial terror, reminiscent of the burning and bombing of sites of Black assembly and resistance such as churches, and indeed, of the burning of victims of lynching. In the days following the fire, people stopped by the cemetery to give new offerings to Nannie.
Memorialization and #BlackLivesMatter
Why has Nannie's grave marker inspired such an outpouring of offerings and attention by scores of people with no direct kinship link to her? Certainly her young age is compelling, as is the approaching storm of national disunion during the span of her life. Perhaps equally significant are the still-ongoing crises of racism and inclusion in the United States. Her prominent, yet plain marker, is suffused with resonance for past and present injustices. The obscurity of her identity allows Nannie to evoke the "many thousands gone" among persons of color in the District and elsewhere. In the present era of #BlackLivesMatter and the continuous assaults on the rights of persons of color to own their bodies, the story of Mount Zion cemetery, nearly eradicated to serve commercial development interests, is particularly resonant. The restoration of this storied African American burial ground, now surrounded by multiples sites of white, elite privilege, is a powerful testimony to African American resilience and cultural vibrancy.


Nannie, for many, has come to represent hallowed ground and the larger history and geography of racial segregation, anti-Blackness, and liberation struggles within the District of Columbia. The centuries-old African-Atlantic practice of grave decoration, ubiquitous in this cemetery in the nineteenth century, has been revived to honor Nannie's memory—poignant testimony to the power of ancestral remembrance—as well as the continuing mission of activism.
About the Authors:
Mark Auslander is the author of The Accidental Slaveowner: Revisiting a Myth of Race and Finding an American Family (Athens: University of Georgia Press, 2011). He is a visiting faculty member in anthropology at Mount Holyoke College.
Lisa Fager, Executive Director of the Black Georgetown Foundation, oversees the Mount Zion and Female Union Band Society cemeteries in Georgetown, Washington DC.
Acknowledgements:
We acknowledge the tireless work and insights of community historians Mary Belcher and Patrick Tisdale, and the many other volunteers associated with the Mount Zion–Female Union Band Society Cemeteries, and the Mount Zion United Methodist Church in documenting the important history associated with the cemetery and the local faith community. Erika Berg located 1894 newspaper accounts of grave decorations in Mount Zion. We are grateful to Carlton Fletcher, Fath Davis Ruffins, Russell Smith, Ibrahim Sundiata, and Jay Ball for many interpretive insights into this narrative. Many thanks to the staff at the Kiplinger Library, Washington historical Society; The Library of Congress Periodicals and Manuscripts rooms; Special Collections and University Archives, The Maryland Room Hornbake Library, University of Maryland College Park; the Smithsonian Institution Archives; the District of Columbia Public Library Washingtoniana/People’s Archive Division and the Georgetown Library Peabody Room; the District of Columbia Archives; the National Archives and Records Administration; the Maryland State Archives; and the Daughters of the American Revolution Library. Particular thanks to Andrew Boisvert of the DAR Library and Damani Davis and Rose Buchanan of NARA Archives 1 for their insights into antebellum District of Columbia records. Omar “Casey" Ibrahim generously shared his memories of recovering the Nannie memorial stone and initiating the modern gift-giving tradition in the 1990s. We are grateful for careful editorial work on this post by Allen Tullos and the Southern Spaces team.
Appendices
]]>
In May of 2023, when the World Health Organization downgraded the coronavirus emergency from a global health pandemic to an "ongoing health crisis," the shift made sense in many ways. Most developed nations have made vaccines available for over two years. Shutdowns and enforced quarantines ended, even in holdout nations. The WHO's announcement signaled that other countries, including the United States, would follow suit if they had not already. This move, however, will have material consequences for grassroots charitable organizations across the US. Endstate ATL (ESA), a group I have worked with since 2021, is one of many non-profit groups that will be affected.
In Georgia, the COVID state of emergency officially ended in May 2022, even as it remained in place at the national level. This allowed organizations like ESA to continue our mutual aid work. But when the US announced the end of the Federal COVID-19 Public Health Emergency (PHE) Declaration on May 11, 2023, enhancements to public assistance and social safety net programs ceased. From this point on, groups like ESA once again will have to jump through multiple bureaucratic hoops to obtain the funding necessary to provide care.
Following the global outbreak of COVID in 2020 many governments created temporary measures to extend aid to vulnerable populations. In the US, these included extensions of unemployment benefits, a moratorium on student loan interest and payments, no-cost COVID testing and vaccinations, Medicare flexibility, and opportunities to provide nontaxable disaster relief funds. The national government also released relief funds to individual state governments, although often these funds did not reach the people who needed them.1Rebecca Riess and Devon M. Sayers, "Alabama Governor Signs Bill to Use Covid-19 Relief Funds to Build Prisons," CNN, October 1, 2021, https://www.cnn.com/2021/10/01/politics/alabama-covid-relief-prison-bills-signed-governor-kay-ivey/index.html. Despite the uneven distribution of aid, many people, specifically children and elders, moved above the poverty line thanks to COVID assistance.2John Creamer, "Supplemental Poverty Measure That Accounts for Additional Government Benefits Lowest on Record at 7.8%," Census, September 13, 2022, https://www.census.gov/library/stories/2022/09/government-assistance-lifts-millions-out-of-poverty.html.

The flexibility surrounding nontaxable disaster relief funds eased mutual aid work. Mutual aid has a long history in the US and Global South, and the onset of the COVID-19 pandemic witnessed an outpouring of community solidarity towards those in need. Mutual aid stands apart from other charity models because of its non-hierachal emphasis on mutualism rather than models that maintain divisions between givers and receivers. Mutual aid is rooted in reciprocity.
Endstate ATL took advantage of these temporary measures for the betterment and aid of our community members. Rooted in southwest Atlanta with a Black queer feminist politic, ESA's work aims to reach those most marginalized through community building, political education, and mutual aid. Through our Black Power Fund, which pays up to three months' worth of utility bills for Black queer households, and our Pack Provides Programs, which provide household supplies, COVID PPE, and infant essentials including formula, clothing, and sanitary products to caregivers of young children, we seek to step in where the state fails to provide support.
Mutual aid allows organizations to provide immediate care and relief to individuals in need without imposing the bureaucratic processes that often keep aid beyond reach. Under a state of emergency, disaster relief payments are not taxable. As such, ESA, and other groups like it, were able to provide direct aid through a less convoluted system of reporting and disbursement. This allowed us to move funds directly and rapidly to people in need and has been crucial to our ability to substantively support people in a timely way. ESA has covered bills for ten households in the past year, as well as covered a year of utilities for the BARRED Business house, which provides stable, community-owned housing for people recently released from prison. We have been able to report these funds as disaster relief.3"Mutual Aid Legal ToolKit," Sustainable Economies Law Center, Accessed June 22, 2023, https://www.theselc.org/mutual_aid_toolkit.








The efforts of mutual aid groups helped supplement aid where state and local leadership failed. Georgia governor Brian Kemp refused to take the COVID-19 pandemic seriously. In 2020, Georgia was the first state in the nation to relax quarantine restrictions, even as Kiesha Lance Bottoms, the mayor of Atlanta, sought to retain many protective measures. Initial reporting that the virus would largely impact the elderly and immunocompromised, combined with anti-fear government propaganda, engendered a sense of invincibility and an attitude of disregard among many Georgians. As of 2021, Georgia had one of the highest COVID mortality rates in the US, and those most impacted were poor, working class, and people of color.4"COVID-19 Mortality by State," CDC, Accessed June 22, 2023, https://www.cdc.gov/nchs/pressroom/sosmap/covid19_mortality_final/COVID19.htm. The refusal of Governor Kemp to implement mandated social distancing or mask requirements, even before vaccines were available, left the entire state population vulnerable to infection. The consequences were devastating, with thousands of unnecessary deaths and debilitating outcomes for those suffering from long COVID.
Pandemic relief payments meant to alleviate the burden of rising interest rates were out of reach for marginalized Georgians. In order to receive national stimulus checks and Kemp's own "special tax credit," individuals needed to have filed and paid taxes for the preceding two years, a barrier that left people who were unemployed or homeless without access to relief.5"Gov. Kemp Announces First Round of This Year's Special Tax Refund," Department of Revenue, May 1, 2023, https://dor.georgia.gov/press-releases/2023-05-01/gov-kemp-announces-first-round-years-special-tax-refund#:~:text=Single%20filers%20and%20married%20individuals,a%20maximum%20refund%20of%20%24500.

In response to the pandemic, groups emerged such as Bed Stuy Strong, based in Brooklyn, which created a robust grocery delivery system by first relying on the resources at their disposal before evolving into a program that benefited thousands.6Haritha Kumar, "Four Key Takeaways from Mutual Aid Organizing During the COVID-19 Pandemic," Georgetown University Beeckcenter, October 4, 2022, https://beeckcenter.georgetown.edu/four-key-takeaways-from-mutual-aid-organizing-during-the-covid-19-pandemic/. Georgia has similar organizations. Community Movement Builders developed stabilization programs that include rent/mortgage payments as well as groceries in their efforts to impede the gentrification of southwest Atlanta, and Food4Lives a non-profit started by Georgia Tech and Emory students provides food and supplies for the unhoused in the greater Atlanta area.7Katie Burkholder, "Housing as a Human Right: Community Movement Builders Organize Against Gentrification," Georgia Voice, April 21, 2022, https://thegavoice.com/today-in-gay-atlanta/housing-as-a-human-right-community-movement-builders-organize-against-gentrification/; "Who are We?" Food4Lives, Accessed June 22, 2023, https://food4lives.org/about.html. Both organizations preceded the pandemic, but their work became much more indispensable in its wake.
The increase in groups doing this aid work was significant, especially in red states where Republican leadership champions laissez-faire government structures for almost everything but reproductive health, policing, and surveillance. Pandemic or no pandemic, people need help. However, smaller aid groups face difficulties in keeping the work going. ESA has primarily been funded by grants, a funding model that is not easily sustainable. According to one of our members, "A significant struggle we've faced since the end of the COVID-19 pandemic is the philanthropic and public perception that the conditions for folks have changed enough that mutual aid is not necessary even as we continue to field a significant number of requests." Further, all members participate on a volunteer basis, spending much of our time otherwise as graduate students, teachers, doulas, herbalists, and nonprofit workers. Over the last two years, many of us have faced our own destabilizing events, financial uncertainty, bouts of COVID, and family loss. The ability of small groups to come together and push to make a difference in their communities—despite personal difficulties and decreasing assistance from governing bodies—should inspire more activism. But the question remains, how can we continue this work when governmental policies have resumed restricting social safety nets while offering few, if any, alternatives?
Changing policy is one problem organizers face, burnout is another. Studies have suggested that we approach "burnout as a part of activism and as influenced by the organizational context, rather than as something that individual activists experience outside of activism."8Maria Fernandes-Jesus et al., "More Than a COVID-19 Response: Sustaining Mutual Aid Groups During and Beyond the Pandemic," Frontiers in Psychology 12 716202, October 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8563598/. However, as young Black people organizing in the South, my colleagues and I experience burnout from many directions. We deal with the stress of everyday life, as well as the difficulty of doing our solidarity work, with constant reminders from government leadership that our goals are at odds with theirs.
With the COVID state of emergency ending in the US, aid provided by organizations such as Endstate ATL becomes taxable, dramatically altering the way funds can be mobilized, as well as the process that recipients must go through to receive support. Charitable tax deductions are reserved for individuals and corporations who donate money to qualified charities.9Up until December 2021, entities meeting these requirements were able to claim as much as 100% of their AGI in charitable tax write offs. "CARES Act Charitable Benefits Not Extended For 2022," Stanford Giving, March 14, 2022, https://giving.stanford.edu/stories/cares-act-not-extended-for-2022/. Because ESA puts money "directly" in the hands of marginalized people, such direct contributions to individuals are not tax-exempt. The COVID state of emergency allowed groups like ESA to move funds to individuals more freely—on an emergency basis. The end of the state of emergency means we must restructure our aid programs. The beautiful thing about mutual aid is that even if one group burns out, another group can and likely will step up right behind to fill the gap. In this way, the work continues. We never stop.
About the Author
Ra'Niqua Lee writes to share her particular visions of love and the South. She earned an MFA in fiction from Georgia State University, and she is currently at Emory pursuing a PhD in late nineteenth/early twentieth century African American literature with a focus on spatial and Black queer feminist theories. Her fiction has appeared or is forthcoming in Cream City Review, SmokeLong Quarterly, Indiana Review, Passages North, Best of the Net 2023, Best Small Fictions 2023, and elsewhere. In 2021, the Georgia Writers Association awarded her the John Lewis Writing Grant for fiction. Her flash collection For What Ails You is forthcoming from ELJ Editions.
Acknowledgments
Many thanks to my colleagues. Without their collaborative support, I would not be able to do this work: Julian Rose, Britni Ruff, Christina Foster, Michelle, Jovan Julien, and extra thanks to Hugh Hunter for his early edits.
Public Health in the US and Global South is a collection of interdisciplinary, multimedia publications examining the relationship between public health and specific geographies—both real and imagined—in and across the US and Global South. These essays raise questions about the origin, replication, and entrenchment of health disparities; the ways that race and gender shape and are shaped by health policy; and the inseparable connection between health justice and health advocacy.
Beginning in 2022, the series expands to include 1000-word blog posts, as well as longer commentaries, essays, articles and media productions that address the public health and political implications of the COVID-19 pandemic from multiple perspectives. The series editor for Public Health in the US and Global South is Mary E. Frederickson.
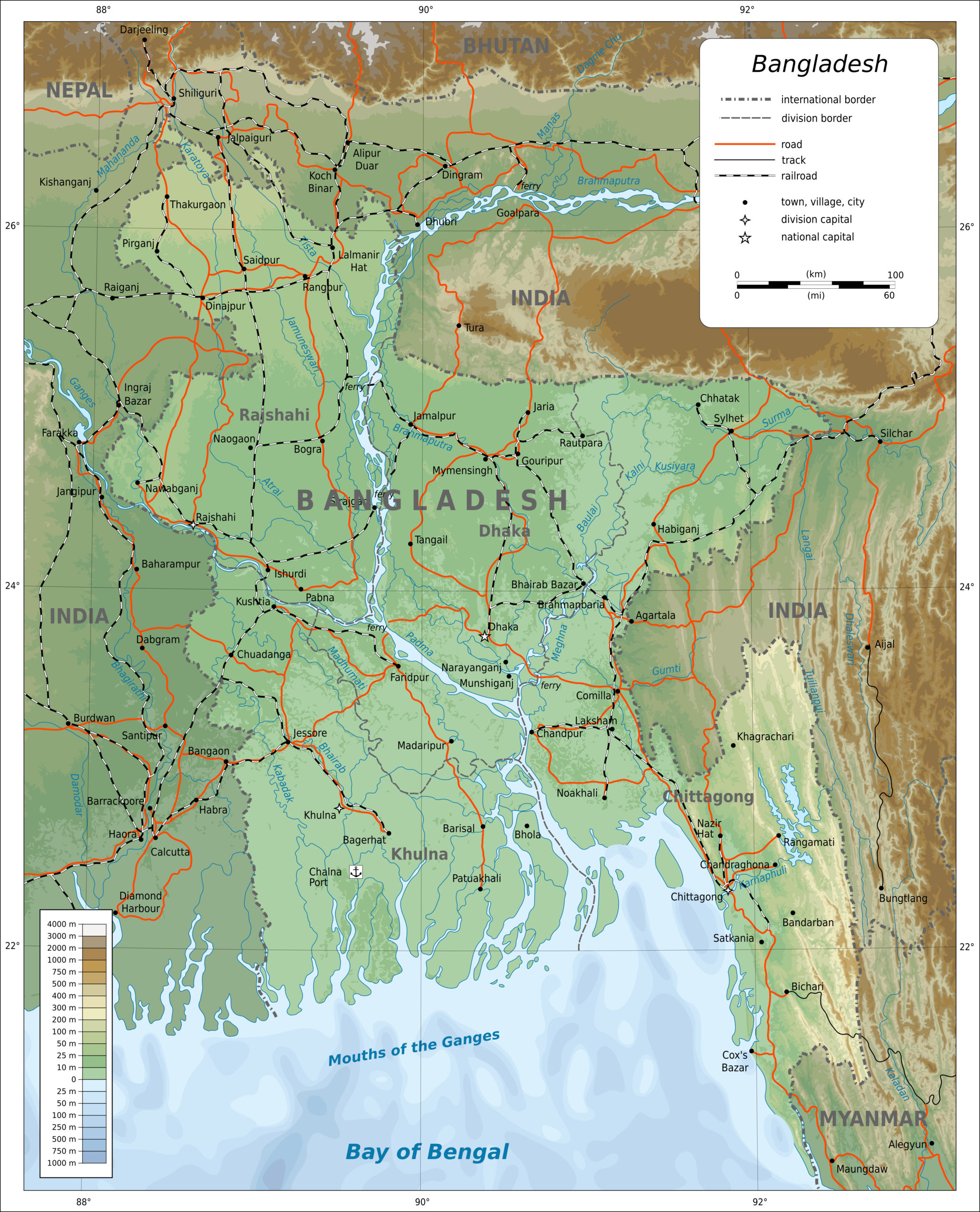
As the world moves into its fourth year since the advent of COVID-19, the pandemic remains a broad public health concern. It is necessary to teach Covid-appropriate behaviors and build public confidence in vaccines and boosters to address new strains of the virus. Across the globe, localized Covid pandemic response projects should complement conventional approaches to preparedness. Community Support Team Dhaka (CST Dhaka) and Community Support Team Cox's Bazar (CST Cox's Bazar) are two projects implemented by the health program of BRAC, a Bangladesh-based NGO.
Bangladesh, the eighth-most populous country in the world (169.4 million people), is a developing country located in South Asia with a 2021 gross domestic product per capita of $2,458. The country has achieved significant progress in reducing maternal, infant, and child mortality rates, decreasing malnutrition, improving immunization coverage, and eliminating infectious diseases like polio. However, it faces emerging health challenges, including the growing burden of noncommunicable diseases, heightened vulnerability to disasters and environmental hazards, and the threat of health emergencies during disease outbreaks such as COVID-19. Bangladesh's health services are centralized and urban-centric.1There are only 1.1 doctors per 10,000 people in rural populations in Bangladesh, while there are 18.2 doctors per 10,000 people in urban areas. Taufique Joarder, Lai B. Rawal, et al, "Retaining Doctors in Rural Bangladesh: A Policy Analysis," International journal of Health Policy and Management 7, no. 9 (2018): 847–858. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6186485/. The country also faces shortages of well-equipped healthcare facilities and healthcare workers. The health financing system in Bangladesh suffers from a lack of adequate funding, absence of appropriate health insurance, and a large dependence (74%) on out-of-pocket payments.
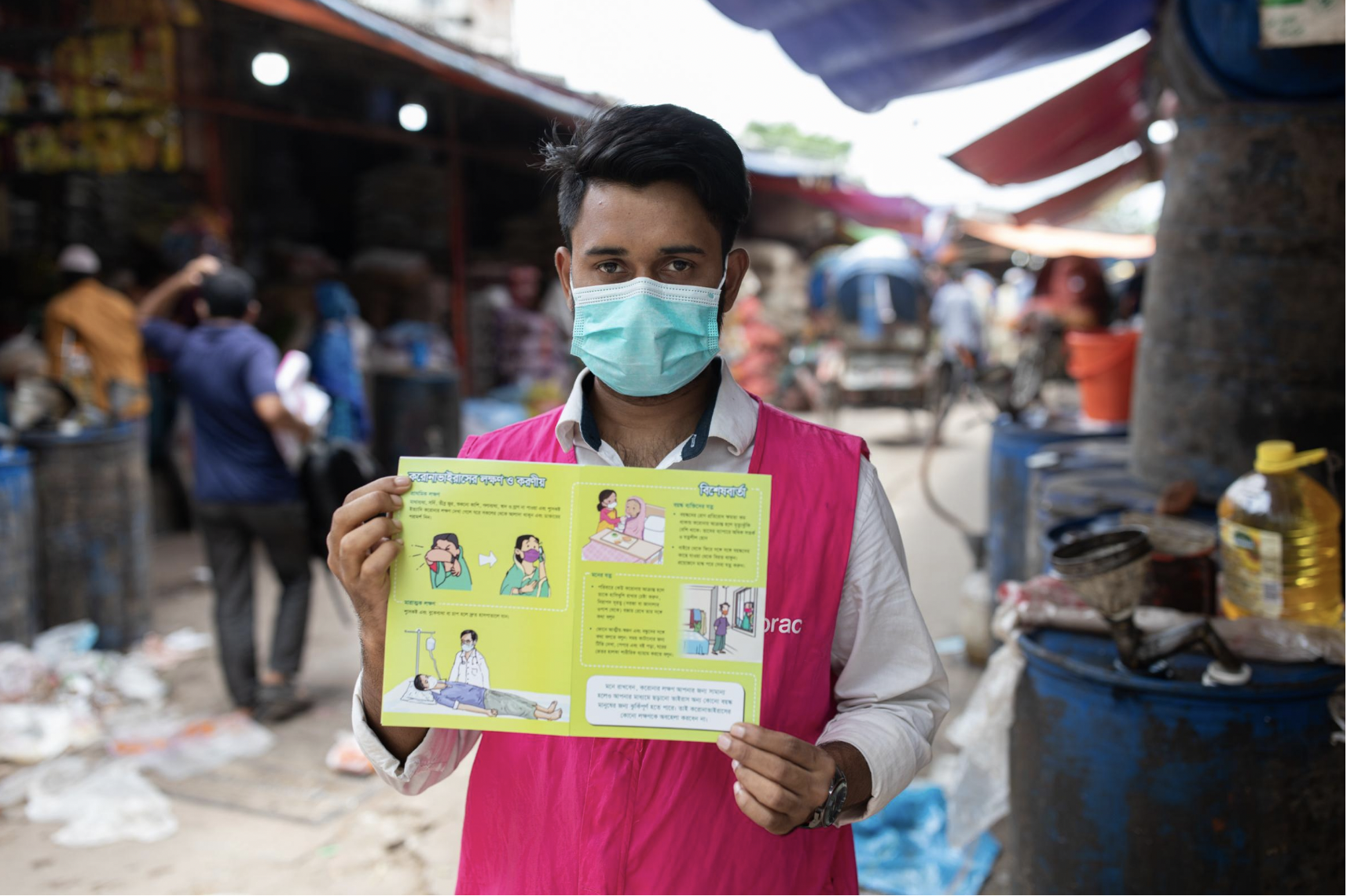
BRAC, founded in 1972, is the largest non-governmental organization in Bangladesh involved in a variety of sectors including public health, education, microfinance, and livelihood support. It currently employs over 100,000 people across Bangladesh and ten countries. Its Health, Nutrition, and Population Programme (HNPP) has been a global leader in developing and scaling up locally-based health worker programs for the rural population. With support from the Foreign, Commonwealth & Development Office (FCDO), the World Bank, and the United Nations Population Fund (UNFPA), the organization implemented two COVID-19 response projects in Dhaka and Cox's Bazar (two of the high-risk districts identified by the World Health Organization after analyzing infection rates in different districts of Bangladesh). BRAC initiated several creative approaches in these locations to tackle the spread of COVID-19 at the height of the pandemic.
"Miking" in Local Dialects

Playing health messages through mobile loudspeakers (locally known as miking) has been around for decades. After the initial round of miking in Cox's Bazar, however, the volunteers and area managers heard from local representatives that the messages in mainstream Bengali were not effectively reaching the people. Here, the Chatgaya/Chittaingya dialect is the primary oral language. Subsequently, the Cox's Bazar project engaged a local voiceover specialist to develop messages in Chittagonian dialect which enhanced the effectiveness of the 849 miking sessions conducted in the region, substantially improving the local population's understanding about vaccination.
Info Cards
A common request received by the field staff (community health workers, volunteers, and area managers) was for comprehensive materials to complement the messages disseminated verbally. In addition to the usual posters, stickers, and leaflets, BRAC designed tri-fold cards with detailed information on vaccination, handwashing, mask wearing and disposal, and instructions about taking care of people with comorbidities. Info cards were distributed to local change-agents such as market committee members or transport hub leaders to help sustain best practices. The cards garnered a positive response from the public.
Collaboration with Sisimpur
As schools in Bangladesh reopened after an eighteen-month shutdown, BRAC collaborated with Sisimpur—a local adaptation of children's television series Sesame Street—in creating an educational video about COVID-19 featuring the Sisimpur characters. Originally developed for the Dhaka project, this video ran on social media platforms and was shown at some three hundred schools. This intervention was entirely novel for many students and schools, and Sisimpur was also warmly received by parents and teachers. Unfortunately, this project began halfway through BRAC's wider Covid education initiatives, and needed more time and closer supervision.
Comics and Murals
Long perceived as reliable messengers in Bangladesh, local artists often translate crucial information into personable and understandable forms. Working with these artists, BRAC delivered COVID-19 information to schools in an engaging way. Renowned cartoonist Morshed Mishu developed wall murals in Dhaka and Cox's Bazar and 200,000 copies of a comic strip were distributed among schools and madrasas.






Faith Leaders' Endorsement
Faith leaders have addressed misinformation and influenced health behavior changes with a high degree of success. During the biggest Ebola outbreak in history, interfaith leaders were instrumental in delivering health messages in parts of West Africa that governments and NGOs could not reach. As credible sources of information, they worked actively on quashing rumors regarding Ebola and encouraged people to listen to government directives and the health workers.2A 2020 study by Afrobarometer revealed that across 34 countries in Africa, faith leaders are more widely trusted than any other public leaders. Brian Howard, "Religion in Africa: Tolerance and Trust in Leaders are High, but Many Would Allow Regulation of Religious Speech," Afrobarometer Dispatch no. 339 (2020), https://afrobarometer.org/sites/default/files/publications/Policy%20papers/ab_r7_dispatchno339_pap12_religion_in_africa.pdf. Early in the COVID-19 epidemic, BRAC teamed up with Islamic Foundation Bangladesh (IFB) and Bangladesh Baptist Church Fellowship (BBCF) to train their directors on best practices. Local representatives of UNICEF, who had previously engaged Muslim leaders in another health project, facilitated the IFB partnership. BRAC provided online training to IFB field supervisors and BBCF pastors via Zoom, addressing questions and rumors. This collaboration provided 3,400 faith leaders with awareness messaging, 860,000 reusable masks, and 350,000 leaflets.




Faith leaders and scholars such as Leor P. Sarkar (General Secretary of the BBCF), Gazi Sanaullah (Islamic scholar), and Pragyananda Bhikkhu (Assistant Director, Ramu Central Sima Bihar) endorsed preventive measures and appeared in short social media videos in support of wearing masks, maintaining social distance, washing hands, and taking vaccines.
While the Dhaka Community Support Team emphasized partnerships with selected faith-based organizations, Cox's Bazar sought to unite all the faith leaders from the intervention areas—Muslim, Buddhist, and Hindu—under one roof for knowledge sharing and collaboration. These meetings included a moderated session that provided equal opportunity to representatives of each religion to share the lessons they had learned. In Ramu, faith-based organizations overcame the silos between their work, meeting to formulate policies for combating the spread of vaccine misinformation. Volunteers working with faith-based groups increased both the reach and acceptance of the interventions.
Faith leader Reverend Leor P. Sarkar speaks on Covid,
Bangladesh. Translated from original Bengali.
Faith leader Gaji Sanaulla Rahmani speaks on Covid,
Bangladesh. Translated from original Bengali.
Interactive Popular Theater
BRAC's popular theater groups under its Social Empowerment and Legal Protection program (SELP), have performed about a wide range of topics such as gender equality, child marriage, violence against women, health, migration, and road safety across sixty-one districts since 1998. To raise COVID-19 awareness, the Cox's Bazar project organized 160 performances, despite dealing with some local challenges. For instance, the acceptance level of popular theatre was lower among the conservative Muslim population and the shows were more difficult to organize in hard-to-reach locations. Social distancing was more challenging when children made up the majority of the audience.

Findings from surveys and focus group discussions indicated increased awareness about COVID-19 symptoms, modes of transmission, and prevention measures (handwashing, mask wearing, social distancing) and vaccination across all intervention areas. Local knowledge about the existence of the virus and its spreadability increased.3Compared to the baseline, 26% more people knew that both hands need to be washed, 11% more people knew not to use a damp or damaged mask, whereas 7% more people knew not to wear the mask loosely. 8% more people reported knowing that the Covid-19 vaccine improves the body's immunity against the virus. School surveys revealed that 10% more students reported that face-to-face communication with the infected was the mode of transmission and almost 4% more knew it could be transmitted through coughing and sneezing. Encouraging accessible, engaging, and equitable approaches to public health communications has led to an increase in the uptake of COVID-19 preventive practices, as well as a reduction in barriers to vaccine confidence.
COVID-19 continues to pose a significant public health concern for many countries, like in India. While Bangladesh faces various health challenges and lacks adequate healthcare facilities and workforce, local NGOs like BRAC have played a significant role in addressing the pandemic's impact through introduction of localized initiatives like miking, info cards, Sisimpur PSAs, comics and murals, and faith leaders' endorsement to strengthen COVID-19 response. Such programs are essential in complementing conventional approaches to pandemic preparedness and mitigating the virus's spread. While these initiatives may be unique to Bangladesh, their successes can provide important lessons for other countries in terms of pandemic response and preparedness.
About the Author
Monzur Morshed Patwary is a public health practitioner with over eleven years of professional experience. As a senior program manager at BRAC, he has led several large-scale projects involving COVID-19 response, maternal and child health, and digitalization of training for community health workers. He has also collaborated with UN organizations and international donors such as USAID, FCDO, DANIDA, and GAC and helped mobilize high-value grants through project design and proposal development. Monzur represents Bangladesh on global platforms such as ParisWHO, Global Leadership Forum and HPAIR Harvard Conference. He completed the Hubert H. Humphrey Fellowship at Emory University-Rollins School of Public Health and is currently pursuing his professional affiliation at The Task Force for Global Health.
Public Health in the US and Global South is a collection of interdisciplinary, multimedia publications examining the relationship between public health and specific geographies—both real and imagined—in and across the US and Global South. These essays raise questions about the origin, replication, and entrenchment of health disparities; the ways that race and gender shape and are shaped by health policy; and the inseparable connection between health justice and health advocacy.
Beginning in 2022, the series expands to include 1000-word blog posts, as well as longer commentaries, essays, articles and media productions that address the public health and political implications of the COVID-19 pandemic from multiple perspectives. The series editor for Public Health in the US and Global South is Mary E. Frederickson.
Commentary
Multiple COVID-19 waves have left in their wake compelling evidence of long overlooked gaps in pandemic readiness and responsiveness. The primary lesson for the US public health and healthcare sectors is that this deep-rooted ignorance took a huge toll on their ability to contend with a novel, rapidly spreading, and lethal contagion. As historian Peter Burke recently noted: "Many vivid examples of the consequences of ignorance come from the history of diseases."1Peter Burke, Ignorance: A Global History (New Haven: Yale University Press, 2023), 189. COVID-19 is a current case in point. What was missed or mismanaged in the run up to the pandemic and during its catastrophic course will, if left unexamined and uncorrected, lead to enormous suffering and loss in additional public health crises. In this commentary, I want to elaborate on how institutionalized ignorance affected the Centers for Disease Control and Prevention's (CDC's) response and what can and should be done to learn from the agency's mistakes, with the goal of avoiding a repetition.

A thorough and fully transparent probe of CDC's recent history is warranted, one that scrutinizes "institutional obliviousness, under a succession of agency directors and programmatic leaders, to basic gaps in readiness and responsiveness that became glaringly obvious during the pandemic and contributed to numerous missteps in the US response to COVID-19."2Daniel Pollock, "COVID-19 Lessons in Ignorance," Southern Spaces, April 28, 2022, the first in a public health series covering the pandemic: https://southernspaces.ecdsdev.org/2022/covid-19-lessons-ignorance/. Far too much had to be cobbled together on the fly in early 2020 largely because of prior organizational neglect. And far too little has changed three years later, even as CDC moves ahead with its latest—to date, largely upper echelon—reorganization.3Centers for Disease Control and Prevention, "CDC Moving Forward Reorganization: A Notice by the Center for Disease Control," Federal Register 88, no. 29 (2023): 9290, https://www.federalregister.gov/documents/2023/02/13/2023-02929/cdc-moving-forward-reorganization.
Yes, SARS CoV-2 is a novel pathogen that spread rapidly, wreaked extraordinary devastation, and evolved quickly. Lots of impromptu learning about the virus and measures to contain or counter was necessary. However, pandemic warning signals abounded for years, and many assets CDC needed to function optimally in public health emergencies—as well as in non-pandemic times—were long overlooked or chronically under supported by virtue of the agency's own strategic planning, programmatic priority setting, and discretionary funding decisions. In surveillance and data science, for example, CDC did not fully mind and mend critically important gaps in electronic case reporting, immunization information systems, forecasting and outbreak analytics, and tools and dashboards for data visualization.
Certainly, factors largely beyond CDC's control had major impacts on the agency's performance. Besides the virus itself, CDC had to contend with (1) a coterie of federal government executives, most notably the 45th President, who failed to respond effectively and exerted unprecedented political interference; (2) a legacy of outbreak responses in the United States that are highly decentralized and contingent on a variety of situational circumstances; (3) longstanding constraints on CDC's public health authorities; and (4) chronic underfunding of public health programs at all levels of government. Each of these factors helps explain limitations, gaps, and shortcomings in the agency's performance. However, to leave the matter there would mean overlooking the impact of internal organizational factors that remain largely under CDC's control. Whether the agency has fully reckoned and responded to its internal problems is an open question that warrants much more attention.

"To be frank, we are responsible for some pretty dramatic, pretty public mistakes, from testing to data to communications," CDC Director Rochelle Walensky acknowledged in August 2022. However, the full CDC Scientific and Programmatic Review report that prompted Dr. Walensky's critique remains under wraps and not publicly available. Many months after the report was completed, all that CDC has published is a high-level summary and set of recommendations.4"CDC Moving Forward Summary Report," Centers for Disease Control and Prevention, Last reviewed September 1, 2022, https://www.cdc.gov/about/organization/cdc-moving-forward-summary-report.html. What was covered in the review, its methods and findings, and how conclusions were reached are shrouded in secrecy. Sequestering the report does not bode well for efforts to learn from CDC's COVID-19 experience and improve the agency's performance. Instead, CDC leaders have opted for a form of knowledge concealment that serves to perpetuate institutionalized ignorance.
For those of us who are deeply concerned about where the agency is headed, this is a fraught moment, yet organizational dysfunctions, mishaps, setbacks, and downturns are not necessarily points of no return. Learning from the COVID-19 pandemic and CDC's response to it can lead to changes that help revitalize the agency. Concealing the recent scientific and programmatic review report is not a good start along the path of organizational learning.

"Organizational learning," according to a leading researcher in the field and her colleagues, "is a process through which experience performing a task is converted into knowledge, which, in turn, changes the organization and affects its future performance."5Linda Argote, Sunkee Lee, and Jisoo Park, "Organizational Learning Processes and Outcomes: Major Findings and Future Research Directions," Management Science 67, no. 9 (2021): 5399–5429. The process should include gathering and moving information across organizational boundaries; eliciting and using multiple viewpoints; acknowledging hierarchies, policies, and practices that have not worked; and trying new approaches that have a higher likelihood of success. A prime example of an opportunity to learn from the COVID-19 experience is reckoning with how the agency organized, staffed, and operated its emergency response. From my perspective, the structure and process defects were profound and persistent, with the upshot that returns on the extraordinary time and effort so many CDC responders committed to their tasks fell well short of what would warrant use of all those precious resources. What purposes did the CDC response serve? Did the agency achieve those purposes? What was necessary to get the job done? Among the more specific questions about CDC's emergency operations is whether all the work involved with preparing, clearing, and presenting extensive PowerPoint slide decks in daily COVID-19 briefings was worthwhile. What were the benefits and at what cost?
Most of CDC's performance problems during the pandemic were the legacy of organizational neglect, not the exigencies of a novel corona virus or other external factors. The botched laboratory test rollout, flawed testing guidance, poorly prepared public health guidelines, confusing messaging, misguided mask recommendations, multiple data and analytic deficiencies, staffing shortfalls, and publication delays are traceable to assumptions widely held within the agency about institutional readiness coupled with longstanding inattentiveness by CDC directors and programmatic leaders to known or partially understood gaps. That CDC was not ready to go live sooner with a publicly facing, state-of-the art COVID-19 data display epitomizes what the agency had neglected. Instead, other data visualization websites, most notably Johns Hopkins University's dashboard, served as the go-to destinations for pandemic surveillance data. The reputational damage to CDC is severe and could have been avoided.
So much had to be launched or improvised by CDC in crisis mode because so much had been taken for granted or ignored for such a long time. Some additional examples from my own experience: When I joined the CDC response as Deputy Incident Manager for data and surveillance at the end of March 2020, I was surprised to learn that the agency had yet to introduce a process to enable secure data access and distribution of COVID-19 data sets to prospective data users who had been identity-proofed by the U.S. Department of Health and Human Services. Further, CDC had taken no steps to inventory and document relevant data sets and make provisions for sharing de-identified data with news organizations, one of which moved forward with a lawsuit to gain access to COVID-19 case data aggregated by CDC. The agency should have closed these basic gaps in data provisioning well before the pandemic, not during the throes of it. The only explanation of this blunder that I can think of is lack of forethought and follow through.

SARS CoV-2 is not the first viral respiratory pathogen to emerge and spread across country borders in the twenty-first century. While each international outbreak has presented a unique mixture of causes and consequences, they also have had much in common. That commonality places a premium on learning from each event and applying take-away lessons in a thoroughgoing way. What's ahead epidemiologically can surpass what's happened already in terms of complexity and magnitude, and that only heightens the stakes for CDC's organizational learning and pandemic preparedness.
While there are many pockets of CDC excellence, the organization, most notably because of its COVID-19 response, has taken multiple hits—some reflect ignorance about the agency's mission, operations, opportunities, and constraints but others are knowledgeable, on target, and of high consequence. There is much to do—and soon. We need to know more about CDC's performance gaps and shortcomings, and how to remedy them. To that end, instead of treating the full details of CDC's COVID-19 mistakes as a sequestered resource, it behooves CDC leaders to build on, transfer, and most importantly, act on what has been learned.6Jeffrey Pfeffer and Robert I. Sutton, The Knowing-doing Gap: How Smart Companies Turn Knowledge into Action (Cambridge, MA: Harvard Business School Press, 2000): 261. In the pandemic's wake, a much stronger commitment to organizational learning by CDC will provide the quickest and most effective solutions to the institutionalized ignorance that placed the public and the agency at risk.
About the Author
After completing the CDC's Epidemic Intelligence Service training program in 1986, Daniel Pollock worked as a medical epidemiologist at the agency for 35 years. Dr. Pollock led the CDC unit responsible for national surveillance of healthcare-associated infections from 2004–2021, and he served in CDC's COVID-19 emergency response in the spring of 2020 as the Deputy Incident Manager for data and surveillance.
Public Health in the US and Global South is a collection of interdisciplinary, multimedia publications examining the relationship between public health and specific geographies—both real and imagined—in and across the US and Global South. These essays raise questions about the origin, replication, and entrenchment of health disparities; the ways that race and gender shape and are shaped by health policy; and the inseparable connection between health justice and health advocacy.
Beginning in 2022, the series expands to include 1000-word blog posts, as well as longer commentaries, essays, articles and media productions that address the public health and political implications of the COVID-19 pandemic from multiple perspectives. The series editor for Public Health in the US and Global South is Mary E. Frederickson.
A case argued in October 2022 concerning Congressional reapportionment in Alabama reveals that the Court's conservative majority is likely poised to follow the lead of Associate Justice Samuel Alito, who in July 2021 wrote the Court's majority opinion reinterpreting the Voting Rights Act's Section 2 to make it more difficult to win a case challenging laws that restrict voting procedures.1 Steve Suitts, "Undoing the Voting Rights Act," Southern Spaces, July 12, 2021, https://southernspaces.ecdsdev.org/2021/undoing-voting-rights-act/.
By further crippling the Act's Section 2, instead of voiding it completely, as the Court did nine years ago to the Act's Section 5 in an opinion by Chief Justice John Roberts involving Shelby County, Alabama, the current Court will reach the same practical result: overturning the ruling of a three-judge court (composed of two Trump-appointed and one Clinton appointed federal judges) that would permit Alabama's Black voters—one-fourth of the state's population—an opportunity to help elect a candidate of their choice in two (not just one) of the state's seven Congressional districts.2Amy Howe, "In 5–4 vote, Justices Reinstate Alabama Voting Map Despite Lower Court's Ruling that It Dilutes Black Votes," Scotusblog, Feb. 7, 2022, https://www.scotusblog.com/2022/02/in-5-4-vote-justices-reinstate-alabama-voting-map-despite-lower-courts-ruling-that-it-dilutes-black-votes/; Merrill v. Milligan, 142 S. Ct. 879 (2022); Shelby County, Ala. v. Holder, 570 US 529 (2013). Steve Suitts, "States Rights Resurgent: The Attack on the Voting Rights Act," Southern Spaces, Aug. 29, 2013, https://southernspaces.ecdsdev.org/2013/states-rights-resurgent-attack-voting-rights-act/.

The case, Merrill v. Milligan, will adversely shape voting rights in Alabama and across the nation, but the worst is yet to come if Justice Alito's remarks from the bench on October 4 foretell the Court's future approach. In an exchange with the US Solicitor General, who sided with Alabama's Black plaintiffs, Alito proffered a couple of far-reaching, deeply flawed notions about voting. If adopted by the Court, they will provide the rationale for further gutting the Voting Rights Act, as effectively as if it were revoked, and for removing federal courts from virtually any future role in protecting Black voting rights in the US South. These are consequences that could be built on Alito's blatant misstatement of facts and blithe misconception of the history of voting rights struggles.
Justice Alito has sought to overturn the Supreme Court's prior cases about reapportionment and voting rights since he was in the Reagan Administration's Justice Department in the 1980s. In his application for a political appointment as Deputy Assistant Attorney General in 1985, he wrote, "In college, I developed a deep interest in constitutional law, motivated in large part by disagreement with Warren Court decisions, particularly in . . . reapportionment."3Mark Sullivan, Memorandum for Mark Levin, Dec. 12, 1985, https://www.archives.gov/files/news/samuel-alito/accession-060-97-761/Acc060-97-761-box1-Alito.pdf. It was in the same application in which Alito that he stated he was "particularly proud of my contributions in recent cases in which the government has argued in the Supreme Court racial and ethnic quotas should not be allowed and that the Constitution does not protect a right to an abortion."
During oral arguments in Merrill v. Milligan, Justice Alito claimed that the current standards used to prove a violation of Section 2 in reapportionment cases were far too easy, allowing Black plaintiffs to win every case or, as he put it, "always run the table" in the South. This assertion is flatly wrong, contradicted by the findings of four noted political scientists who filed a brief in the Alabama case. They told the Court that during the last twenty years, there have been only thirty-one lawsuits claiming dilution of minority voting in the redistricting of the legislative seats of fifty states and 435 Congressional districts. But, only nine of the thirty-one challenges have prevailed in federal courts.4Transcript of Oral Argument, Merrill v. Milligan, US Supreme Court, Oct. 4, 2022, 105, https://www.supremecourt.gov/oral_arguments/argument_transcripts/2022/21-1086_6j36.pdf; Brief of Amici Curiae Jowei Chen, Christopher S. Elmendorf, Nicholas O. Stephanopoulos, and Christopher S. Warshaw In Support of Appellees/Respondents, Merrill v. Milligan, July 18, 2022, 7–8, https://www.supremecourt.gov/DocketPDF/21/21-1086/230239/20220718132621523_91539%20HARVARD%20BRIEF%20PROOF3.pdf. The brief notes that these numbers do not include settlements. Also, the brief reports that earlier in the 1990s 43 Section 2 challenges to district plans involved twenty-two of them in favor of plaintiffs.

Even if Alito and his law clerks had not read the brief, he could not fail to hear Justice Sonya Sotomayor cite the same statistics minutes earlier during oral argument. "Section 2 is not being used that widely," she noted, quoting the brief's statistics as she made the point that cases were brought and won "only in an extreme circumstance where voters are polarized completely and where there's no crossover between the races."5Transcript of Oral Argument, Merrill v. Milligan, 71–72.
Alito would have none of these facts. He claimed that the current test for proving a Section 2 violation meant Alabama would never win a reapportionment case. "They're not going to win on whether the minority group is politically cohesive. They're not going to win on whether the majority votes as a bloc," he charged.6Transcript of Oral Argument, Merrill v. Milligan, 105. In other words, Alito contended that Black plaintiffs would always win a case because they always could prove that white voters in Alabama cast most of their ballots as a bloc and that their bloc-voting rarely, if ever, included support for the candidates of Black voters, who also usually voted as a cohesive group.
But, according to Alito, Black plaintiffs ought not win the cases because the bloc-voting by both Black and white people "may be due to ideology and not have anything to do with race. It may be that voters and white voters prefer different candidates now because they have different ideas about what the government should do."7Transcript of Oral Argument, Merrill v. Milligan, 105. Simply put, Alito suggests it is an ideological, partisan difference, not a racial difference, that can explain why white voters usually reject and defeat the Black voters' candidates of choice in districts where white voters are in the majority.
Alito's observation echoes the outline of an argument that the national Republican Party is aggressively advancing to disable the Voting Rights Act. The National Republican Redistricting Trust (NRRT), the primary Republican organization coordinating national, state, and local Republicans in every state's Congressional and state legislative redistricting, filed a friend of the court brief in the Alabama case. It claims that the Voting Rights Act "intended to equalize minority voting opportunities has instead become a cudgel wielded against any state law that fails to advance the institutional interests of the Democratic Party."8Brief of Amicus Curiae The National Republican Redistricting Trust in Support of Appellants/Petitioners, Merrill v. Milligan, May 2, 2022, https://www.supremecourt.gov/DocketPDF/21/21-1086/222354/20220502163340023_21-1086%20and%2021-1087%20Amicus%20NRRT%20Supp.%20Appellants.pdf.
The NRRT brief cites an earlier lower court opinion from Alabama where US District Court Judge Keith Watkins decided that in the statewide elections for state supreme court justices "factors other than race—most prominently, partisan politics and the decline of the Alabama Democratic Party" explain the election outcomes.9Ala. State Conference of the NAACP v. Alabama (M.D. Ala. Feb. 5, 2020), Case 2:16-cv-00731-WKW-SMD Document 181, 100. The Black plaintiffs lost the case.
Southern Republican leaders are also beginning to parrot this claim. For example, Republican US Representative Troy Nehls of Texas (author of The Big Fraud, in support of former President Trump's claims of a stolen election) recently told the New York Times that the majority of white voters in his Congressional district were not voting against the minority communities' candidate: "These people aren't against brown or Black people. They just don't like the way Democrats are running the country."10Michael H. Keller and David D. Kirkpatrick, "Their America Is Vanishing. Like Trump, They Insist They Were Cheated," New York Times, Oct. 23, 2022, https://www.nytimes.com/2022/10/23/us/politics/republican-election-objectors-demographics.html.
Alito's Republican-inspired argument, if adopted by the Supreme Court, would be devastating to voting rights cases. In 2019 the Court held in a case concerning North Carolina's Congressional reapportionment that federal courts cannot become involved in partisan gerrymandering since it would involve the courts in allocating power among the political parties.11Rucho v. Common Cause. 139 S. Ct. 2484 (2019). An essential part of winning a Section 2 lawsuit against a reapportionment plan requires proving that most white voters in majority-white districts routinely do not vote for the candidate whom Black voters support. In this way, bloc voting by white voters on account of race effectively denies Black voters an equal opportunity to participate in electing candidates to office in violation of the Voting Rights Act. But, if courts begin to decide that bloc voting by whites is based on partisan politics, instead of race, there can be no case heard by the federal courts about voting rights.
Not even the state of Alabama was brazen enough to make this claim, although it did make its own shameless argument in its brief as to why the Court ought not consider the effects of racial bloc voting. "Racially polarized voting is not state action," the state of Alabama claimed. It is the actions of private citizens and therefore outside the reach of the Constitution which only restricts government actions.12 Reply Brief for Appellants/Petitioners, Merrill v. Milligan, Aug. 24, 2022, 37–38, https://www.supremecourt.gov/DocketPDF/21/21-1086/234404/20220824160744143_Merrill%20-%20Merits%20Reply%20Brief%20FINAL.pdf. This is an old, discredited notion. Segregationists of the 1940s argued unsuccessfully that the Democratic party's primary elections in the South were private primaries of private political parties, not state action, uncontrolled by the Constitution or the courts. Of course, the Supreme Court flatly rejected that claim since the Court understood that southern officials were using a non-governmental political party's all-white primary as an essential tool in the state government's plan to minimize the impact of Black voting.13Smith v. Allwright, 321 US 649 (1944).
The assertions of the Republicans and Justice Alito are no less ancient and discredited. Southern white leaders have attempted to intimidate, limit, and deny Black people's voting ever since they gained the right to vote because Black citizens have held a different political ideology. In 1867, for example, the first "Alabama Colored Convention" endorsed the Republican party and as new voters proclaimed a political ideology that included "education secured for all; with the old and helpless properly cared for; with justice everywhere impartially administered."14Lucille Griffith, Alabama: A Documentary History to 1900 (Tuscaloosa: University of Alabama Press, 1968), 461. The following year, the executive committee of the all-white Democratic and Conservative Party of Alabama announced its opposition to the state's Reconstruction Constitution, which sought the Black Convention's political agenda, which included universal, adult voting and free schools for all children financed by a set aside of one-fifth of the state annual revenues.
The conservative white Democrats insisted, "Color or race has nothing to do with the motive of any one in withholding political privileges." They wrote that it was only because too few Black voters embraced "the science of civil policy to cast an intelligent vote, wisely favor or oppose a legislative measure" that they opposed the new constitution and Black voting.15"To the People of Alabama," Jacksonville (AL) Republican, Oct. 24, 1868, 2.
When conservative whites, including the Ku Klux Klan, burned Black schools and churches in Alabama and across the South during Reconstruction, their defenders claimed it had little or nothing to do with race—only political differences. "As a rule the schoolhouses (and churches also) were burned because they were the headquarters of the Union League and the general meeting places for Radical politicians," wrote Walter L. Fleming in 1905, "or because of the character of the teacher and the results of his or her teachings."16Walter L. Fleming, Civil War and Reconstruction in Alabama (New York: Columbia University Press, 1905), 628.
Later, along with other southern states, conservative white Democrats in Alabama disfranchised Black voters in the state's 1901 constitution not merely because they were formerly enslaved Black people. They disfranchised them because Black voters had joined with white Republicans and Populists to challenge conservative white Democratic candidates in pursuit of a different political agenda.17C. Vann Woodward, Origins of the New South, 1877–1913 (Baton Rouge: Louisiana State University Press, 1951), 321–331. Of course, it involved "different ideas about what the government should do" between most white and Black people, and partisan differences. But it was also rank racism.
Similarly, Alabama Governor George Wallace's opposition to Black voting, which eventually helped to enable passage of the Voting Rights Act in 1965, was based on race, but it also involved a partisan fear that the "bloc vote" (as he called Black voters) would join with a minority of white voters to defeat his political agenda at the ballot box.18Steve Suitts, A War of Sections: How Deep South Political Suppression Shaped Voting Rights in America (Athens: University of Georgia Press, 2023).
There is no way to forecast if Justice Alito will attempt to incorporate his Republican-serving rationalizations into the Alabama case or if other members of the Court will follow him in constituting a majority in this case or another. What is clear is that by continuing to dismantle the nation's foremost protections of Black citizens' right to vote and their right to have their votes count equally in election outcomes, a majority of US Supreme Court Justices, often in the name of color-blindness, will be blind to the political history of racism in the Deep South—or will knowingly misconstrue it with an apparent partisan result.
About the Author
An adjunct with Emory University's Institute for the Liberal Arts, Steve Suitts is the author of the A War of Sections: How Deep South Political Suppression Shaped Voting Rights in America (Athens: NewSouth Books, an imprint of the University of Georgia Press, 2023). Earlier in his career, Suitts served as the executive director of the Southern Regional Council, vice president of the Southern Education Foundation, and executive producer and writer of "Will the Circle Be Unbroken," a thirteen-hour public radio series that received a Peabody Award for its history of the civil rights movement in five Deep South cities.
]]>Commentary
As a public health professor at the University of Michigan, I've encountered opinions about the Covid vaccine in my own family that reflect mistrust and hesitancy. I can understand this.1Melissa Creary, "Bounded Justice and the Limits of Health Equity," Journal of Law, Medicine & Ethics 49, vol. 2 (2021): 241–256; Creary, "Legitimate Suffering: A Case of Belonging and Sickle Cell Trait in Brazil," BioSocieties 16 (2021): 492–513; Creary, "Biocultural Citizenship and Embodying Exceptionalism: Biopolitics for Sickle Cell Disease in Brazil," Social Science & Medicine 199 (2018): 123–131; Melissa Creary, Paul Fleming, Sheeba Pawar, and Amel Omari, "Leading with HEART: Working Toward Health Equity with Anti-Racist Teaching," The Pursuit, University of Michigan School of Public Health, April 29, 2021, https://sph.umich.edu/pursuit/2021posts/leading-with-heart.html; Creary, Paul Fleming, Trivellore Eachambadi Raghunathan, "The Impact of Race on Data." University of Michigan Population Healthy Podcast, February 16, 2021, https://sph.umich.edu/podcast/season3/the-impact-of-race-on-data.html; Creary and Anne Pollock, "How COVID-19 has highlighted racism as a health risk." King's College London Podcast, June 11, 2020, https://www.kcl.ac.uk/news/how-covid-19-has-exposed-racism-as-a-health-risk. Like many Black households in the US, my family had little reason to "trust the science," especially that produced during the presidency of Donald Trump, who consistently endorsed racist policies and spewed racist rhetoric.2Karen Grigsby Bates, "Is Trump Really That Racist?" NPR, October 21, 2020, https://www.npr.org/2020/10/19/925385389/is-trump-really-that-racist. While the public health response in the United States to COVID-19 was uneven across federal, state, and local entities, the narrative about disproportionate risk and mortality became apparent early and the public health establishment eventually sprang into action to make a case for health equity in the deployment of testing, prevention, and care.3Tasleem J. Padamsee, Robert M. Bond, Graham N. Dixon, et al, "Changes in COVID-19 Vaccine Hesitancy Among Black and White Individuals in the US," JAMA Network Open 5, no. 1 (2022), https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2788286. A survey published in January 2022, found that COVID-19 vaccine hesitancy had decreased more rapidly among Blacks than among whites since December 2020. Researchers found that Blacks "more rapidly came to believe that vaccines were necessary to protect themselves and their communities."
Even with these efforts, many of my family members initially could not be persuaded to take the vaccine. I was increasingly frustrated and wished they had more faith in science. Yet, even though I was vaccinated, I shared some of their concerns, and as I've written: "how can people who have never experienced equity be trusting of a supposedly new urgent call for equity when it comes to the vaccine?"4Fabiola Cineas, "Black and Latino Communities are Being Left Behind in the Vaccine Rollout," Vox, February 24, 2021, https://www.vox.com/22291047/black-latino-vaccine-race-chicago. If there were a culture that recognized a right to healthcare, would my family feel the same way? If we expected the state to have responsibility for our health and if we had a history of the public health system systematically and consistently providing preventative treatments and care, regardless of partisan politics, would it make a difference in vaccination rates in the present crisis?
In addition to studying health justice and equity in the United States, I have researched health policy development in Brazil. Segments of the Brazilian Black Movement in the 1990s, modeled to a significant extent on the 1960s US Civil Rights Movement, demanded the right to healthcare. Black participants in my Brazilian study deployed policy-based attempts to achieve full access to citizenship—most prominently as a right to health rights.5Creary, "Bounded Justice," 241–256. My work in Brazil explored how patients, non-governmental organizations, and the Brazilian government, at state and federal levels, have contributed to the discourse of sickle cell disease (SCD) as a black disease, despite a prevailing cultural ideology of racial mixture. Drawing on ethnography and oral histories from Rio de Janeiro, Salvador, Brasília, and Porto Alegre, this project charts the simultaneous constructions of race and science through SCD across Brazil. When I lived in Brazil in 2013, I was struck by just how much everyday people, within social movements and as part of civil societies, called on the Brazilian state to manage and provide healthcare access. With this in mind, I compare the public health systems in the United States and Brazil, the right to public health, and the COVID-19 vaccine.
The rollout of Covid vaccines in the United States was painfully slow. The Trump administration's Operation Warp Speed broke records in vaccine development in 2020, but floundered badly when it came to distributing immunizations in early 2021. President-elect Biden set the goal of deploying 100 million vaccinations in the first 100 days of his administration, pledging to streamline delivery throughout the nation. Shots went into arms and by mid-March 2021, a quarter of the population had received at least one vaccine; six months later that number rose to 85 percent.
Although Black Democrats were vaccinated at a lower rate than white Democrats, the values associated with vaccine hesitancy follow the lines of partisan values and ideological orientation. A Michigan study in early 2021 found the following:
. . . in the initial wave of the outbreak in May 2020, Blacks experienced more severe direct impacts: they were more likely to be diagnosed or know someone who was diagnosed, and more likely to lose their job compared to Whites. In addition, Blacks differed significantly from Whites in their assessment of COVID-19's threat to public health and the economy, the adequacy of government responses to COVID-19, and the appropriateness of behavioral changes to mitigate COVID-19's spread. Although in many cases these views of COVID-19 were also associated with political ideology, this association was significantly stronger for Whites than Blacks.
The study found that Black Michiganders had more at stake, and more to lose. They were more likely to be infected with COVID-19, so they were also more likely to adopt behaviors of compliance. A history of racist mistreatment, however, affected their compliance. Those who perceived the impact of COVID-19 as less threatening were less willing to comply with mitigating behaviors. The Michigan study demonstrates how that state is a microcosm of the United States. According to data from mid-2021, the top twenty-two states with the highest adult vaccination rates voted for Joe Biden in the 2020 presidential election, and some of the least vaccinated states were the most pro-Trump. This partially explains the influence that Trump had (and arguably still has) on perceptions of vaccine validity and necessity.
But major resistance remained: in September 2021, 35 percent of the eligible US population remained unvaccinated and of that group, 83 percent said they did not plan to get the lifesaving shots. By the end of 2021, 73 percent of adults eighteen and older had received at least one dose of a Covid vaccine, however, 27 percent remained unvaccinated. Of those, 42 percent reported that they "don't trust the vaccine." Vaccine hesitancy, racial inequities in distribution, and state and local disparities in healthcare funding and facilities, continued to impede vaccine delivery as first the Delta variant and then Omicron took their deadly and debilitating toll.6Staff, "A Timeline of COVID-19 Vaccine Developments in 2021," AMJC, June 3, 2021, https://www.ajmc.com/view/a-timeline-of-covid-19-vaccine-developments-in-2021.
In contrast to the Covid geographies of the US, Brazilians appeared to "love vaccines," as Lucas Fontainha wrote in Undark, a digital magazine exploring the intersection of science and society. "They fight for vaccines," he continued, "they throw vaccine festivals, they kiss all the babies in the line waiting for vaccines, they camp overnight at the clinic to get a vaccine . . . even the anti-vaccination Brazilians vaccinate in secret."7Kiratiana Freelon, "Opinion: In Brazil's Successful Vaccine Campaign, a Lesson for the U.S," Undark, October 14, 2021, https://undark.org/2021/10/14/in-brazil-successful-vaccine-campaign-lesson-for-us/.

Unlike Americans in the US, Brazilians have benefitted from robust public health programs and a strong vaccine infrastructure since the 1970s. That said, throughout the pandemic, Brazilians have had to contend with Jair Bolsanaro, the "Trump of the Tropics," a man filled with authoritarian vitriol and disregard for vaccine science. Many worried that his influence would deter vaccine uptake, especially because 55 percent of the country voted for him. Bolsanaro's sphere of influence remains significant. His lukewarm stance on Covid vaccines and his refusal to pre-order them in 2020 and early 2021, resulted in many deaths. Nevertheless, a citizenry that believes healthcare is a basic right has countermanded Bolsonaro's failure of leadership. As the number of Brasilians dying from Covid increased to over 600,000 in 2021, citizens largely ignored their president, eschewed their free choice option to not vaccinate, and lined up for the shots.8Felicia Marie Knaul, Michael Touchton, Héctor Arreola-Ornelas, et al, "Punt Politics as Failure of Health System Stewardship: Evidence from the COVID-19 Pandemic Response in Brazil and Mexico," The Lancet Regional Health: Americas 4 (2020), https://www.thelancet.com/journals/lanam/article/PIIS2667-193X(21)00082-X/fulltext.
In 1973, Brazil created a national immunization program (Programa Nacional de Imunizações) that led to the near-eradication of polio and measles by 2000.9"National Immunization Program–Vaccination," Ministry of Health, accessed July 6, 2022, https://www.gov.br/saude/pt-br/acesso-a-informacao/acoes-e-programas/programa-nacional-de-imunizacoes-vacinacao. This successful program has been strengthened by the creation of a universal healthcare and public health system (Sistema Único de Saúde or SUS) that invested (in-part) in the delivery of free public healthcare, including vaccinations to every Brazilian, codified by the Brazilian Constitution of 1988.10Jairnilson Paim, Claudia Travassos, Celia Almeida, et al, "The Brazilian Health System: History, Advances, and Challenges," Lancet 377, no. 9779 (2011): 1778–97, https://pubmed.ncbi.nlm.nih.gov/21561655/. Vaccine delivery to Brazilian citizens is integrated into everyday life and normalized through informal connections, familiarity, and hyper-locality. Although Bolsanaro rejects the idea that the nation state owes a responsibility to its citizens, the state and local arms of the government (and the Constitution), disagree.11Vincent Bevins, "Despite Bolsonaro, Brazil Has Barely Any Anti-Vaxxers," Intelligencer, November 10, 2021, https://nymag.com/intelligencer/2021/11/despite-bolsonaro-brazil-has-barely-any-covid-anti-vaxxers.html. Not only is the state obligated by law to distribute free services and pharmaceuticals, but citizens are mandated to be part of the process. Even those who choose private insurance must get their vaccines at SUS.














{kind=link}
{kind=link}
Even when an anti-science president such as Bolsonaro rails against vaccines, there is almost no way for the population to avoid receiving inoculations. In August 2021 in the city of São Paulo, the campaign Virada da Vacina reported that 99 percent of the adults in the city had been vaccinated (Bolsonaro won approximately 45 percent and 60 percent of the vote here in the run offs and general election respectively).12Isabella Menon and Paulo Eduardo Dias, "São Paulo Approaches 99% of Adults with the First Dose of the Covid Vaccine," Folha De S.Paulo, August 15, 2021, https://www1.folha.uol.com.br/equilibrioesaude/2021/08/sao-paulo-se-aproxima-de-99-dos-adultos-com-a-primeira-dose-da-vacina-contra-a-covid.shtml; "See the Calculation Map of all Cities in Brazil," Fohla De S.Paulo, October 7, 2018, https://www1.folha.uol.com.br/poder/eleicoes/2018/veja-o-mapa-de-apuracao-de-todas-as-cidades-do-brasil/?#/cargo/presidente/local/sao-paulo/turno/1/mapa/estadual/municipio/sao-paulo/3550308. Six-hundred locations dispersed the vaccine; sixteen of these were open for walk-in or drive-up around the clock. The state provided DJs, dancing, bands, and artists on stilts to create a carnivalesque atmosphere for those waiting hours in line.
Vaccine culture in Brazil is about accessibility. Locals become part of the campaign. That means you are likely to know and have some regard for the person who comes to you in the name of immunization—in the metro stations, on street corners, or in the park. Public displays boost the vaccine's image. It is harder to retreat into spaces of disinformation when the people you know, or even don't know, seem open to receiving a vaccination. A 2021 study showed that even among vaccine-hesitant individuals in Brazil (10.5 percent of the sample), only 2.5 percent did not intend to vaccinate at all.13Daniella Campelo Batalha Cox Moore, Marcio Fernandes Nehab, Karla Gonçalves Camacho, et al. "Low COVID-19 Vaccine Hesitancy in Brazil," Vaccine 39, no. 42 (2021): 6262–6268. Still, a June 2022 report from The Lancet found that municipalities that supported Bolsonaro in the 2018 elections were those that had the worst COVID-19 mortality rates, especially during the second epidemic wave of 2021.

As of June 2022, 87.3 percent of Brazilians have received at least one dose of COVID-19 vaccine and 79 percent have been fully vaccinated, compared with 79.8 percent of US citizens having received one dose and 67.5 percent being fully vaccinated.14COVID-19 Vaccination Tracker, Reuters, last updated July 15, 2022, https://graphics.reuters.com/world-coronavirus-tracker-and-maps/vaccination-rollout-and-access/. While these numbers are not vastly different, it is of note that Brazil President Bolsonaro remains in power, regularly flouting vaccine regulations and bragging about his unvaccinated status, whereas since 2021 in the United States, President Joe Biden has worked tirelessly to get vaccines in arms, bolster public health, and eliminate health disparities.15Rodrigo Pedroso, "Brazil's Bolosnaro Says He Will Not be Vaccinated Against Covid-19," CNN, October 13, 2021, https://www.cnn.com/2021/10/13/americas/bolsonaro-no-vaccine-intl/index.html; Chuck Todd, Mark Murray and Carrie Dann, "Biden is True to a Key Promise: Getting More Shots in Arms," NBC News, March 19, 2021, https://www.nbcnews.com/politics/meet-the-press/biden-true-key-promise-getting-more-shots-arms-n1261531; HHS Press Office, "Biden-Harris Administration Provides $121 Million in American Rescue Plan Funds to Support Local Community-Based Efforts to Increase COVID-19 Vaccinations in Underserved Communities," HHS, July 27, 2021, https://www.hhs.gov/about/news/2021/07/27/biden-harris-admin-provides-121-million-in-arp-funding-to-local-communities-for-covid-19-vaccines.html.
Early in his tenure, Biden proposed a $1.6 billion increase for the Centers for Disease Control and Prevention to improve core public health capacities in states and territories, modernize public health data systems, train new epidemiologists and other public health workers, and build global capacity to respond to future health threats. Some of these efforts have worked. By August 2021, Pew research reported that around three-quarters of US adults (73 percent) had received at least one dose of a COVID-19 vaccine.
Despite these efforts, too many Americans see vaccine mandates, not as a way toward building public safety, but as extreme government overreach. Republicans and Libertarians have called repeatedly and loudly for "personal freedom" to be prioritized over public safety. Before the Supreme Court blocked the Biden administration's vaccine-or-test requirement for large private businesses in January 2022, there was an outcry for #massnoncompliance. Some scholars have called this political resistance to vaccines based on the tenets of choice and liberty, a "uniquely American predicament."16Alana Wise, "The Political Fight Over Vaccine Mandates Deepens, Despite their Effectiveness," NPR, October 17, 2021, https://www.npr.org/2021/10/17/1046598351/the-political-fight-over-vaccine-mandates-deepens-despite-their-effectiveness. And while the oppositional forces of conservatism and science have been noted as phenomenon elsewhere, including Brazil, the lack of a dominant US culture that trusts and respects public health and expects that the state can and should deliver it can be attributed largely to decades of right wing ideologues across many forms of media.
To date, an Omicron subvariant (BA-5) is the newest variant of concern, threatening a wave of infections and reinfections. As we continue to navigate this global pandemic, we must pay attention to the true influencers of public health. In Brazil, the public health system has a strong history of emboldening citizenry with a message of governmental duty and obligation. We'll see how this may play out in the polls come October for upcoming elections in this country. In the United States, anti-vax politicians, many of whom have themselves received the vaccine for COVID-19, have spread misinformation and anti-government rhetoric about public health. Although conservatism and evangelical religiosity has led to vaccine hesitancy, a Pew Report shows us that most Americans who go to religious services say they would trust their clergy's advice on COVID-19 vaccines. Some advocates of public health have historically prioritized local partnerships with religious leaders and institutions acknowledging this very important sphere of influence.
We must continue to undertake hard conversations about the tensions between individual freedoms and population health much as we did when H1N1 struck our collective shores. As families like my own navigate the implications of a mutating virus that generated a global pandemic, we need trusted resources that are sensitive to historical experiences and the collective common good.
About the Author
Dr. Melissa S. Creary is assistant professor in the Department of Health Management and Policy, School of Public Health at the University of Michigan and the senior director for the Office of Public Health Initiatives at the American Thrombosis and Hemostasis Network (ATHN). She assists ATHN in finding ways to leverage public health research and policy to make a broader impact within the bleeding and blood disorders population. Dr. Creary's areas of specialization include race and racism, genetics, identity politics, health policy, and health equity. She worked for a decade as a health scientist at the Centers for Disease Control and Prevention in the Division of Blood Disorders, has done extensive field work in Brazil, and has more than twenty years of bench, public health, and social science research experience.
Public Health in the US and Global South is a collection of interdisciplinary, multimedia publications examining the relationship between public health and specific geographies—both real and imagined—in and across the US and Global South. These essays raise questions about the origin, replication, and entrenchment of health disparities; the ways that race and gender shape and are shaped by health policy; and the inseparable connection between health justice and health advocacy.
Beginning in 2022, the series expands to include 1000-word blog posts, as well as longer commentaries, essays, articles and media productions that address the public health and political implications of the COVID-19 pandemic from multiple viewpoints. The series editor for Public Health in the US and Global South is Mary E. Frederickson.
Commentary
An online search using the keywords "COVID-19" and "lessons" turns up an astonishing volume and assortment of information: thousands of commentaries, news stories, scholarly articles, book chapters, and monographs. The lessons are intended for vast expert and general audiences: from pediatricians, public health professionals, and other specialized communities of practice to ordinary people and political leaders across the planet. What has been, can be, and should be learned? More lessons loom. Expect a deep dive Congressional investigation and blue-ribbon probes. Storytellers are weighing in with fictional chronicles. Booker Prize winner Ian McEwan's novel, Lessons (New York: Alfred A. Knopf, 2022), is scheduled for September 2022.

From my perspective as a recently retired Centers for Disease Control and Prevention (CDC) branch chief who served in the agency's COVID-19 response from late March through June 2020, the profusion of "lessons learned" reflects the magnitude of the knowledge gaps that impaired America's readiness and undercut its efforts to grapple with a new pathogenic peril, one for which danger signs were long evident. Failures in foresight were followed by fitful attempts at comprehending a lethal contagion's spread and knowing what to do about it.1Cormac Bryce, Patrick Ring, Simon Ashby, and Jamie K. Wardman, "Resilience in the Face of Uncertainty: Early Lessons From the COVID-19 Pandemic," Journal of Risk Research 23, no. 7–8 (2020): 880–887.
The story of the nation's COVID-19 plight is as much an unfolding epistemological crisis as it is a once-in-a-century epidemiological catastrophe. Among the many lessons to be distilled are how and why ignorance in various forms and places accounts for so much of what went wrong. A thorough and wide-ranging exploration is needed, which calls for contributions from multiple disciplines and approaches. As historian of science Robert Proctor recommends: "We need to think about the conscious, unconscious, and structural production of ignorance, its diverse causes and conformations, whether brought about by neglect, forgetfulness, myopia, extinction, secrecy, or suppression."2Robert N. Proctor, "Agnotology: A Missing Term to Describe the Cultural Production of Ignorance (and Its Study)," in Agnotology: The Making and Unmaking of Ignorance, ed. Robert N. Proctor and Londa Schiebinger (Stanford, CA: Stanford University Press, 2008), 1–33. Further, as sociologist Scott Frickel suggests, we also need to focus on "how, where, and why ignorance, once produced, becomes institutionalized."3Scott Frickel, "Not Here and Everywhere: The Non-production of Scientific Knowledge," in Routledge Handbook of Science, Technology, and Society, ed. Daniel Lee Kleinman and Kelly Moore (New York: Routledge, 2014), 263–276. For example, studies of CDC's shambolic performance should include close scrutiny of institutional obliviousness, under a succession of agency directors and programmatic leaders, to basic gaps in readiness and responsiveness that became glaringly obvious during the pandemic and contributed to numerous missteps in the US response to COVID-19.
If the so-called Spanish influenza of 1918 was, in the words of historian Alfred W. Crosby, America's Forgotten Pandemic, then for the time being the bounty of lessons suggests that COVID-19 is America's Teachable Moment Pandemic.4Alfred W. Crosby, America's Forgotten Pandemic: The Influenza of 1918, Second Edition (New York: Cambridge University Press, 2003), 311–328. The largest public health cataclysm in a hundred years has put to the test assumptions, capacities, decisions, practices, and policies. In many ways, the United States has been found wanting, as evidenced by the exceptionally devastating and inequitable toll that COVID-19 has exacted, much of which was averted or more proficiently mitigated by other countries, including nations in the Global South. Vietnam is a prime example.

Events turned US exceptionalism on its head; the nation's heralded public health preeminence ran aground against a novel corona virus. Remarkably, four months before the World Health Organization declared the worldwide spread of COVID-19 a public health emergency, preparedness experts convened by the Nuclear Threat Initiative and Johns Hopkins University reported that the United States was at the top of the heap internationally in terms of its readiness to contend with a pandemic. Scoring 83.5 out of 100 possible points, the US was deemed "best prepared" in the world.5Elizabeth E. Cameron, Jennifer B. Nuzzo, Jessica A. Bell, et al, Building Collective Action and Accountability, GHS Index, October 2019, https://www.ghsindex.org/wp-content/uploads/2019/10/2019-Global-Health-Security-Index.pdf. Yet, when the virus began to spread throughout the nation, political and public health leaders overlooked or failed to respond promptly and effectively to signals of a mounting threat.
Myriad displays of ignorance in preparedness and response cast a spotlight on areas of knowledge, most visible in America's contributions to pathogen genomics and vaccine development, that were the rarity rather than the rule. As historian Peter Burke predicts, much will be said about ignorance when we look back on the pandemic.6Ana R. Rego and Marialva Barbosa, "Interview With Peter Burke: About Ignorance Nowadays," Revista Famecos—Midia, Cultura e Tecnologia 28 (2021): 1–7. The United States will provide many examples for review. "The coronavirus is very much under control in our country," President Donald Trump claimed without justification in February 2020.7"Trump Says Coronavirus Is 'Very Well Under Control' in U.S.," Bloomberg, February 25, 2020, Video, 1:26, https://www.bloomberg.com/news/videos/2020-02-25/trump-says-coronavirus-is-very-well-under-control-in-u-s-video. When cases and deaths surged, corporate America chimed in with commercials proclaiming "we are all in this together," a slogan that blithely disregarded systemic, inequitable differences in exposures, resources, and outcomes.8"Every Covid-19 Commercial is Exactly the Same," Microsoft Sam, April 15, 2020, YouTube video, 3:40, https://www.youtube.com/watch?v=vM3J9jDoaTA. As COVID-19 variants emerged and disease waves swelled, public health officials justified shifts in their response guidance with the catchphrase "follow the science," in effect denying knowledge gaps and glossing over judgment calls that informed their decisions.9Nason Maani and Sandro Galea, "What Science Can and Cannot Do in a Time of Pandemic," Scientific American, February 2, 2021, https://www.scientificamerican.com/article/what-science-can-and-cannot-do-in-a-time-of-pandemic/. Sports celebrities and other influencers joined in; some publicly declined vaccinations for spurious or unspoken reasons. In one widely publicized instance, a National Football League Most Valuable Player invoked vaccine misinformation to justify his decision to remain unvaccinated.10Ken Belson and Emily Anthes, "Scientists Fight a New Source of Vaccine Misinformation: Aaron Rodgers," New York Times, November 14, 2021, https://www.nytimes.com/2021/11/08/sports/football/aaron-rodgers-vaccine.html. These displays of ignorance, from the individual to the federal levels, almost certainly will be among the major topics covered when histories of America's recent past are written and discussed.
To a large extent, first drafts of our national COVID-19 history have been assembled, produced in near real-time amid an evolving pandemic. Among the lengthier accounts are books by Nicholas Christakis, Scott Gottlieb, Michael Lewis, Andy Slavitt, and Lawrence Wright.11Nicholas A. Christakis, Apollo’s Arrow: The Profound and Enduring Impact of Coronavirus on the Way We Live (New York: Little, Brown Spark 2020); Scott Gottlieb, Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next Pandemic (New York: HarperCollins, 2021); Michael Lewis, The Premonition: A Pandemic Story (New York: W.W. Norton, 2021); Andy Slavitt, Preventable: The Inside Story of How Leadership Failures, Politics, and Selfishness Doomed the U.S. Coronavirus Response (New York: St. Martin’s Press, 2021); Lawrence Wright, The Plague Year: America in the Time of Covid (New York: Alfred A. Knopf, 2021). Their narratives and additional reports, published across a wide variety of media platforms and outlets, recount a now familiar cascade of main events: warning signals missed or ignored. Contagion risks initially misunderstood or minimized. Testing bungled. Weaknesses in public health infrastructure and operations laid bare. Guidance delayed, shifted, and politicized. Mandates and masks applied, albeit unevenly. Healthcare stretched to the breaking point. Inequalities exposed. Supply chains disrupted. The economy slackened. Government spending skyrocketed, then dipped. Red-Blue divides widened. Vaccines produced in record time received mixed receptions. COVID-19’s impact surged, subsided, and swelled again—repeatedly. The pandemic dragged on and left its mark virtually everywhere and on everyone.
A bevy of initial accounts present a broad historical outline of what happened—to date. However, potential pitfalls arise when these first reports go beyond chronicling pandemic events and enter the realm of causal interpretations and lessons learned. There, the authors of quick-to-publication stories should tread particularly carefully, recognize uncertainties, and avoid unjustified or imbalanced explanations. Possible missteps include ignoring explanatory information or information sources and failing to acknowledge, or minimizing, the limits of their evidence. The risks of missing the mark are substantial. Causal interpretations skewed towards the unequivocal and unnuanced provide unreliable takeaway lessons and often obscure deeper etiologic factors. Revisions may be forthcoming, but inaugural versions can exert an outsized influence on what endures as the conventional understanding of what happened and why.

A case in point and cause for concern is Michael Lewis's bestselling The Premonition: A Pandemic Story (New York: W.W. Norton, 2021), a fast-paced narrative—a Hollywood movie version reportedly is on the way—that tells the tale of several outside experts who tried to spur CDC insiders to recognize and respond rapidly in early 2020 to signals of the brewing COVID-19 calamity. CDC's performance leaves little doubt that the agency was ill-prepared for the pandemic and made multiple mistakes in its response, including its botched diagnostic testing roll out, guidance fiascos, and acquiescence to political pressures from the White House. The open questions that Lewis takes on are what accounts for these failures and, more broadly, the poor showing by the United States compared with its lofty, pre-pandemic preparedness ranking. His answers are uncomplicated and unequivocal: the talents and recommendations of experts, represented by a small but heroic crew of scientists and physicians whom he profiles, were ignored, and the underlying cause was a lack of public health leadership, exemplified by the failings of the Trump-appointed CDC Director. According to Lewis, Donald Trump himself bears little responsibility for America's anemic response. "As one of my characters puts it," Lewis reports, "Trump was a comorbidity."12Michael Lewis, The Premonition: A Pandemic Story (New York: W.W. Norton, 2021), xiv.
I read Lewis's book closely, concentrating on his account of CDC's poor performance and the lessons to be learned. Notwithstanding his mystifying minimization of Trump's baleful role, Lewis's The Premonition offers a glimmer of hope for revelatory explanations and guidance. "After a catastrophic season, management always huddles up to figure out what needs to be changed," he suggests in his introduction, invoking a football analogy that promises a line of sight into the gap between reputation and results.13Lewis, xv. However, the front office managers are the target rather than the truth tellers in Lewis's narrative.

To tell his story, Lewis mainly relies on a small coterie of outside experts, most prominently a retired Sandia National Laboratories senior scientist who studied the effects of social distancing on mitigation of pandemic influenza, a former assistant director of the California Department of Public Health who warned state officials about the mounting COVID-19 threat during the pandemic's initial phase, and two physicians who helped write a national pandemic preparedness and response plan during the George W. Bush administration and raised early alarms about COVID-19's potentially devastating impact on the United States. High among their recommendations for thwarting a rapidly spreading contagion were school closures, which Lewis describes as one of the "truths" that his informants had discovered long ago.14Lewis, 211. Yet, considering the downsides of school shutdowns and remote learning, cleaving to that plan and putting it into practice in the COVID-19 pandemic was far from an unequivocal success, an important lesson that eludes Lewis and warrants much further attention.
Lewis doesn't make clear whether he sought or used information from CDC responders about the agency's performance. Notably, he doesn't mention any contact efforts or interviews with insiders about CDC's emergency operations. The enormously harmful effects of Trump and his minions were clear to me and many CDC colleagues, as were major internal weaknesses in the agency's response, which Lewis largely ignores. Some of CDC's shortcomings were due to acute managerial and resourcing problems, often recurring or persistent despite multiple attempts at remediation; others reflected longstanding internal and external assumptions, refuted by the agency's woeful performance, about institutional readiness, proficiency, and sustainability in a pandemic. We need fuller accounts of what went wrong and why, including contributions by CDC insiders, to correctly cull lessons and put them to good use.
More broadly, the flaws in Lewis's assessment serve as a reminder that knowledge claims presented as takeaway lessons do not necessarily undo our ignorance. Some "lessons learned" ignore or minimize more compelling understandings of what went wrong and obscure what we ought to know better. The epistemological crisis that compounded the epidemiological calamity threatens to continue in new forms with the writing of pandemic histories and production of Hollywood dramatizations. Still, COVID-19 has the potential to propel high-value learning and positive changes at the individual, organizational, and societal levels.
Among the nation's earliest and most important pandemic lessons is the immense toll that ignorance can take on human lives. As I write this conclusion, American COVID-19 deaths are fast approaching the one million mark, and untold numbers of people who survived the acute phase of their infections are affected by long-term sequelae. Perhaps we now know better the enormity and implications of what was missing in the national efforts to contend with the pandemic, and we will address collectively what science and technology scholar Manjari Mahajan aptly describes as the "complex political and social determinants that anchor a country's public health response and that are critical in ensuring the sustained well-being of a population."15Manjari Mahajan, "Casualties of preparedness: the Global Health Security Index and COVID-19," International Journal of Law in Context 17, no. 2 (2021): 204–214. COVID-19's impact also has been evident in other, more individual lessons and actions. For many Americans, the pandemic has prompted a personal reckoning and welcome revisions in how they take care of themselves and other people in their lives. However, many COVID-19 lessons and changes are likely to fade, including some that are well worth preserving. America's Forgotten Pandemic of 1918 is a prime example of the finite limits on attention spans and memories. In our time, military conflict and other crises or preoccupations are likely sources of competition for mindfulness, efforts at sense making, and shifts in priorities and routines. "Information is no longer a scarce resource," notes sociologist Sheldon Ungar, "attention and interest are."16Sheldon Ungar, "Ignorance as an Under-Identified Social Problem," British Journal of Sociology 59, no. 2 (2008): 301–326. As a result, America's COVID-19 lessons, including those that are forthcoming, are at risk of diminution or disappearance regardless of their value.
The pandemic is a uniquely teachable moment in our history; we can learn from our ignorance and act accordingly. As political scientist Eric Stern reminds us, despite the formidable obstacles to learning from a crisis, great benefits can accrue from lessons that are deeply reflective, methodologically sound, and highly pragmatic.17Eric Stern, "Bridging the Crisis Learning Gap: From Theory to Practice," in Organizing After Crisis: The Challenge of Learning, ed. Nathalie Schiffino, Laurent Taskin, Céline Donis, and Julien Raone (Brussels: P.I.E. Peter Lang, 2015), 257–272. COVID-19 has made ignorance and its negative consequences more visible in America. Fortuitously, at least for the time being, our lessons in ignorance also provide an impetus for new knowledge and, hopefully, momentum towards a more equitable society, stronger commitments to public health and healthcare, and a much greater responsiveness to planet-wide threats.
About the Author
After completing the CDC's Epidemic Intelligence Service training program in 1986, Daniel Pollock worked as a medical epidemiologist at the agency for 35 years. Dr. Pollock led the CDC unit responsible for national surveillance of healthcare-associated infections from 2004–2021, and he served in CDC's COVID-19 emergency response in the spring of 2020 as the Deputy Incident Manager for data and surveillance.
Public Health in the US and Global South is a collection of interdisciplinary, multimedia publications examining the relationship between public health and specific geographies—both real and imagined—in and across the US and Global South. These essays raise questions about the origin, replication, and entrenchment of health disparities; the ways that race and gender shape and are shaped by health policy; and the inseparable connection between health justice and health advocacy.
Beginning in 2022, the series expands to include 1000-word blog posts, as well as longer commentaries, essays, articles and media productions that address the public health and political implications of the COVID-19 pandemic from multiple viewpoints. The series editor for Public Health in the US and Global South is Mary E. Frederickson.