
Southern Spaces: Oh, here's Michelle now. Are you in your RV?
Michelle Fishburne: Yes, I am. As a matter of fact, I'm in the RV at Jordan Lake State Park near Chapel Hill. It's about ten minutes from where I raised the kids. I have a twenty-three-year-old who has struggled with long COVID, but has just graduated from UNC. And then we'll go up to Princeton, New Jersey, where I grew up. I'll be housesitting for two weeks.
Q: We've been intrigued by your book, Who We Are Now. It's an important project. The interviews hit powerfully with regard to the loss and heartbreak from COVID. Sometimes now, in the wake of the pandemic, it's possible to think it wasn't really that bad. Life goes on. But going back to the beginnings and to the following many months as you do, the power of this pandemic can't be avoided.
Let's start with what were you doing when it became evident COVID had arrived and was not going away. What were the early months of COVID in 2020 like for you? When was it evident that COVID was not going to be a two week, stay-home-and-then-go-back-to-life-as-normal situation? And how did you develop the project that ultimately became the book?
Fishburne: I think that moment when I realized this was going to last more than two weeks takes me into early April. In January, I had just gotten back from a wonderful vacation in Grand Cayman and I had told everybody all over holiday break how much I was enjoying my job and that I could just pinch myself. It was just a great job. I was a public relations partnership person for Inmates to Entrepreneurs, some people who really, really needed it. I was working on an event at the US Senate and the House of Representatives. We were talking to John Legend, who was working on something similar, about going into a prison with him.
And then on January 17, an unknown virus attacked my eighth cranial nerve and I lost my hearing in my right ear and my vestibular functioning. I began using a walker and learning to adjust to life without hearing in one ear. In February, I bought a prom dress for my senior in high school. She was very excited about the prom and we were waiting to hear back from colleges.
Then my boss, when he saw COVID coming, he was having some struggles. His doctor said to him, "You know, you can't go anywhere." And so he said to me, "I'm going to have to lay you off because I can't go do any of these things that you are preparing." So I was laid off and I thought, "No big deal. I have a law degree from UVA. I have had an illustrious career. I've done wonderful things. I'll find a job." I wasn't panicked. But I submitted eighty-six customized cover letters between the middle of March and the middle of July, and I had nothing.
The lease on the post-divorce house was coming up on July 31. I knew that on August 1 I would have no house, no spouse, no job, and no kids to take care of. And the big critical moment happened in a Target parking lot on June 15, when I had to decide where to have the movers put my stuff. I thought, "What doesn't make any sense for me is to rent a place because I have no idea where I'm gonna have to go to get a job. I've got the motorhome that I homeschooled my kids in for ten months once. All right, I can move into the motorhome." So I put everything in storage.
And then I thought, "Oh, what will I do? Well, I love the Outer Banks. Take the motorhome to the Outer Banks." But then I thought, "Michelle, you can be in hell while you're in paradise. And if you're waking up every day thinking what's your next job, you're kidding yourself. You need a project."
I could drive out to Yellowstone from North Carolina because I've done it before. Yeah, and then I will cry the entire time I go to national parks because I won't be with my little ones anymore and I'll be all by myself.
Then out of the blue came the idea of Humans of New York. And I thought, "Oh, Brandon Stanton interviewed thousands of people in New York, took their photo, got a little snippet of their story, put it on social media." I could do the same thing. I could do Americans of the pandemic. Who We Are Now—that was the name right from the beginning.
I know that when you focus on other people, it's easier not to be afraid. I also know now from somebody I met during the interviews that action is the antidote to fear.
Getting in the motorhome and doing a fast run helped with my fear. And focusing on other people helped with a different kind of fear. But I was also very naive. What made me think I could go out in the middle of the pandemic and find strangers to talk with?
Q: Your project started off the way interviews work. One person leads to another. But you say that your fear did not seem to have been pandemic related. We're wondering, weren't you concerned about catching the virus?
Fishburne: I wasn't. Once again, naivete really helped. I thought, "I'll just wear my mask and I'll be smart. I mean, I could be smart in Chapel Hill. Why can't I be smart in Saint Louis or New Mexico?" But what I found when I got out into parts of the country that were sparsely populated, I started to reconsider what critical thinking meant.
I did take some risks. I'd think, "Okay, this building is big enough and it's just me and this person. They're way over there and I'm way over here." Because if somebody is going to tell you a story, and they've just met you, and it's about their lives, especially since I only ask one question, what I really needed was for somebody to keep going and going, going and going, right in my face. Inviting them to continue and showing interest. The mouth is really important to that. As much as I tried to use just part of my face and some body language, there were times when I needed to take off the mask.
Q: That makes perfect sense. So you talk about how this book got started, but then you traveled a long road. How did you have the momentum to sustain the project?
Fishburne: It became something unto itself. I'm just a project person and I got in the groove. What sustained me was how surprised I was every single time I got to listen to somebody else. I mean, there were genuine moments of surprise in every single interview. For example, when I talked with Anne, who's the wedding planner in LA, I had in my mind all these questions I was going to ask her because I was interested in how weddings had changed. But when I asked her the one question, she went off in a completely different direction that surprised me.
I think the excitement of knowing I was going to hear somebody else's story is what sustained me.
Q: Who was most helpful in encouraging and supporting you?
Fishburne: My mother, who is now eighty-five, was my sounding board and supporter. She also is an editor. I would send her transcripts of the interviews. I would think, "Well, this person's got different parts of their story in different places in this transcript." So I would move it around then send it back to the person and ask, "Is this what you said?" Or they'd say, "Yes, that's pretty much what I said. Or, "I said 'like' too many times. Can you take that out?"
My mom has a PhD in sociology from NYU. I grew up knowing about qualitative and quantitative research. Knowing how you ask the question is so important. We talked about the question a lot. And I needed to have a grid, a mosaic, to do a representation of the US as best I could. We talked about that, too.
Q: How did you organize your project? And, to get a sense of the scale and the scope of all the interviews you did, how much is included? How much is left out? How did you edit?
Fishburne: I was conscious of what was going on geographically. Age, race, gender, class, they're all in the mosaic. Urban, suburban and rural. Religion of different kinds. There's New York City and there's Jackson, Mississippi. I used a reverse order of population of the top fifty cities to make sure that I got different types of urban places in different parts of the country.
One area I leaned into heavily was the performing arts because they rely on a live audience. And other vocations that really had a hard time. I overloaded those a bit because they were compelling.
I interviewed about three hundred people, but only a hundred are in the book. There are more on the website and there are more that never made their way into a story. One of the peer reviewers called the book "elegiac," not a word I had anticipated. He had seen the book without any photos. Originally the contract was for forty photos, but one hundred people. And I thought, "I don't know how I'm going to choose which forty people." This was December 2021. My editor at UNC, Lucas Church, said, "Maybe we shouldn't have photos in the book. Then it would be elegiac." So the book went without the photos; the way it's set up, it kind of tumbles.
In order to get that tumble feel, some of the stories had to be very short. For example, I spent two hours with Luke and Rodney and only used Luke's story about how he got more grief for wearing a mask than holding the hand of his partner. Lucas said the stories need to be between 250 words and about 1,200. The average interview was probably thirty-five or forty minutes. If the average story length is six-hundred words, which takes about three to five minutes to say out loud, the book has about five hundred minutes of material. And I recorded three-hundred times thirty minutes. A lot was left out.
When Who We Are Now was published—I'm just going to say the truth—it did not do very well. We think what happened is that it arrived during COVID exhaustion. Yeah. More recently, the couple of book clubs that have used it have really delighted in it because it helped them reframe what the pandemic was. I know that however-many-years hence everything that I gathered is going to have more value than it has today. I think in seven years, when I'm sixty-seven, I'm going to be a very popular lady at the ten-year anniversary.
Q: As a historical read as compared with a contemporary read, I think you may not have to wait that long.
Fishburne: Sometimes when I pick it up and I read it—like I just opened up to Tina, the grief counselor—it washes over me. It all just comes back and you think, "Oh, yes, we had to go through that. How do you grieve when you can't have the formal process?"
And then when I was re-reading Tina's story, Melissa's story in Corinth, Mississippi came flooding back. Her mom had died during COVID. And Melissa said to me, "I've always thought it odd when a family member passes and you go back to the home and you have the whole spread of food that people bring. I never understood the importance of it until now. Because now when I walk down the street, it can be a beautiful day, months and months after my mom has passed and I'm having a good day and somebody who hasn't seen me since my mom passed will say, 'Melissa, I am so sorry about your mom.' I didn't get the kind of closure you get with everyone there eating food, drinking, talking."
And in a way that's how it was with COVID itself. It came, peaked, and petered out, but we never had the "end," even though the federal emergency was over. But it's not the end. Especially for people with long COVID.
Q: You mention that Who We Are Now came out around the time of COVID fatigue. But how did these oral histories affect you? Did you compartmentalize them as research?
Fishburne: I didn't see the project as research. It was just my life. Even now, when people talk about the pandemic, most people talk about it in ways that are very foreign to me. And the way I talk about it is very foreign to most people. Before I got in the motorhome and drove around the country, I thought I knew the pandemic experience, but that was based on my own lived experience. When I left here in September 2020, I expected to find desolation, depression, and division. I expected it to be very, very negative. What really surprised me was the human tenacity. The pluck. And that's the word that I use now a lot, pluck, which is spirited and determined.
In doing the interviews, I settled on asking only one question: What was your 2020 supposed to be like and what did it end up being? And people could talk about what they wanted to. They talked about what really mattered to them, what really defined this period of time, and what made it very difficult, or challenging, or surprising.
People who were out in areas that are sparsely populated would say, "Oh, I just went on the same way." But I know having been there, that every person was changed during the pandemic. More than normally every person genuinely thought about other people and what they were going through. And then there were people who were not given anywhere near the support they needed.


Q: And what do you say now, with a bit of distance, in terms of the perspective that you have?
Fishburne: My mom keeps telling me that I'm a sociologist and I keep pushing back and saying, no, I'm a collector of stories because a sociologist goes back and looks writ large. And I don't feel qualified to do that. I centered the project on individuals and offered up each story.
Many people had very difficult experiences of having to go in and try to do their jobs under incredibly hard circumstances. Often, they didn't have the equipment, didn't have the guidance, didn't have the support. They were watching people die or people turned people away. They couldn't do the jobs that they had trained to do. Then people would come in and reject what they were trying to do or tell them they were wrong. That was head spinning. Or to walk into a store and nobody would have masks on because it was a state where you didn't need to have a mask. It was like a horror movie. They'd think, "Which one of you am I going to see next week?" A lot of the people that I talked with in the healthcare field felt like they went through a trauma.
I thought about various groups of people who were struggling. For instance, I talked with Emma, a director of a migrant farmworker nonprofit. She told me about how really nobody cared to protect migrant farmworkers and about one man who died alone in a motel room. That never should happen. In Birmingham, I interviewed Anne, who was running a homeless shelter. She said it got to a moment when she had to ask whether people were safer inside the building or outside.
I had just started eastward in Texas when Governor Abbott announced that you didn't need to wear a mask anymore. I'm like, "What the heck, Texas is a long state to have to go through no matter which way you do it, right up or down or sideways." I was going west to east and had to be in the state for four more days. It became very uncomfortable. I am a political animal so it was really hard for me to not lean into that. But I became so fascinated with each individual. And I thought, "We are all in this together."
But let's take Fox News, on cable all over America right now. And I was really angry at a big part of the country. I'm like, how can you think that way? How can you think that way? It's Fox News. People have had it in their homes for so long. Fox was pitting us against each other, making people angrier and angrier. Some really ugly parts of us came out. But when you actually get in and talk to people, that's not who they want to be. That's not what they want to be thinking about it.
The false narrative that COVID was not as serious as it indeed was really impacted our healthcare workers and public health officials. I interviewed people who had significant responsibilities, including top public health officials in major metropolitan areas, and they stepped away or are in therapy. And some decided not to deal with it affirmatively. One doctor I spoke with recently said, "I can't talk about it." She started the dialogue and then she said, "I can't. I've just put this away in a compartment. I just can't touch it. I just can't do it." But then, there was a nurse who cried at the end of the interview and said, "Oh my gosh, I just really needed to talk about that."
I saw and heard America in these different ways. People trying to get through. It was such an odd time. The challenges we faced were very unusual.
Luke, South Carolina
Mask Wearer—November 2020
We have felt more discriminated against for wearing masks than being gay. And that's crazy. In the United States of America, we are getting more nasty comments said to us in a grocery store, on the street, for the fact that we have a mask on than the fact that we're holding hands as two men. That's just hilariously tragic. Like, that's where we're at? You're really going to be angry that I have a mask on? So no shame or foul to people who don't want to wear a mask—just don't call me a sheep because I have a mask. That literally happened to me at the gas pump this week.
Valerie, North Carolina
State Senator—December 2020

On March 3, I was attending a conference in Charlotte, and I got a text message from Health and Human Services. It was, to put it mildly, surprising to get a text from DHHS out of the blue. They were alerting me that the first confirmed cases of coronavirus in the state of North Carolina were in my district. Two residents of Chatham County who had traveled to Italy had contracted the disease. I knew enough to know that this was huge and that we were on our way into something that was not going to be good. I left Charlotte that day rather than staying over the next night because I knew that if there were two cases, there certainly were more.
When I look back at 2020, coming from that point of entry into where we are now, with massive unemployment because of shutdowns, and then the blowback, the pushback, it has been very, very difficult. We knew the shutdowns were not the best thing for the economy, but having this juxtaposition of the economy versus overall healthy communities was hard. The governor was in a tough position.
And in the midst of all of that, we were waiting on the federal government to bring in aid. When people started to lose their jobs and people's rents and mortgages and car payments went into jeopardy, there was no help. And the state system was not equipped to handle the massive number of unemployment insurance claims. Before COVID, we usually had about 800 or so claims a week. Then all of a sudden, we went from 800 to 1,800 to 300,000.
Our constituents were coming to us saying, "I followed everything you told me, Senator. I filed my unemployment claim and I've waited for three weeks now. When I call, nobody answers the phone. When I go online, I get knocked off. When I do stay online, I keep getting the same thing saying I'm not eligible. I know I'm eligible. I can't pay my rent and my family is going to be out on the street. Can you help me?"
How many of those folks do you think I could help? Very few. And then the small businesses were calling and saying, "Senator, we're not eligible for PPP [Paycheck Protection Program]." Or "Senator, you can only apply through certain banks or lending institutions. I've never done this before. I need technical assistance in applying." Or "Senator, I don't have an established relationship with this bank, so they will not even talk to me. So where's our help?" That's so painful.
And then I got the call that brought everything really close to home. It went like this.
"Hey, Valerie, how are you?"
"I'm good, how are you?"
"Not so good. So-and-so died of COViD."
"No, can't be."
"Yes."
"What happened?"
"Well, you know he had surgery. After the surgery, he was sent to a convalescent center. He contracted COVID there and died in four days."
Two days later, his family asked me if I would eulogize him. The ceremony was on May 2. There was no church service, just a graveside service, because of course we had to be outside. Afterwards, my husband and I just drove around because I just was not ready to go inside. While we were driving, I got a phone call. I had noticed at the funeral that my friend's best friend was not there. Well, so I got the call from another friend who was at the funeral. This is how it went:
"Valerie, I know this is going to upset you, but they found Kenneth dead today."
"What do you mean?"
"That's why he wasn't at the funeral."
He was only two years older than me. Kenneth was the editor and publisher of the Carolina Times newspaper, one of the few Black newspapers in our state. So that's no more. That's the end of an era that started with his grandfather, Louis Austin, way back in 1927.
And so, when I quiet myself, those are the things I most vividly remember.
Frank, Louisiana
COVID-19 Ventilator Patient—January 2021

I was working for a nonprofit organization driving a bus. We would bring older people, people on Medicare, back and forth to doctor appointments, rehab centers. I come home from work, sit down, and watch TV, and all of a sudden, I can't breathe. I called my son and he took me to the hospital. They diagnosed me: "You have COVID." I said, "Man, I ain't got no COVID." The next morning, Dr. M. come and say, "What's the matter?" I'm telling him I come here last night, and the doctor told me I have COVID. I just couldn't breathe. He said, "Are you ready to go home?" I said, "Yeah." So they let me come home. Got home, next day, the same thing. Can't breathe.
They had an ambulance service come get me. They came in here and gave me a breathing treatment and took me to the hospital. And when I got there, on March 24, Dr. M. say he's going to put me in a medically induced coma. I went to sleep on March 24 and when I woke up, it was April 23. I'd been on a ventilator for almost thirty days. The hospital's head of infectious medicine told Dr. M. to unplug me earlier than that, but Dr. M. said, "Man, I'm in the business of saving lives. I'm not going to unplug that man and tell his family he is brain dead, which he's not." When I woke up, I asked my wife when was Easter, and she said, "Boy, Easter been gone." And I say, "Where I been?" And she said, "You been out, asleep." But I didn't remember nothing, and I didn't realize how sick I was until I called my wife and said, "When you come get me?" and she said, "Not right now." I had no idea that I couldn't walk. I had no idea. I couldn't go to the bathroom. I couldn't pull up in the bed. I couldn't use nothing on my body. Hands, legs, feet, nothing. I couldn't do nothing, period, in a vegetative state. I lost the use of everything, man.
They told me they would send me to a rehab center. When I got there, they put me in a room, and the next thing I know, they put me on a second floor by myself and told me that I got COVID again. So I stayed thirty days in there, with everybody masked up, aproned up, gloved up. And they just got me laying there in the bed, can't turn over, can't feed myself, can't do nothing. And nobody could come visit me because I was in isolation. Every time they come in the room, they'd say, "Why are you down in that hole?" "Man, I've been trying to get out of this hole, but I don't have the strength to pull myself up." And then they get mad with you, they'd bring three or four people in and take you out of the hole and then all of a sudden you're back in that hole. Yeah, I mean, I'm laying flat like this for three months. It was supposed to be a rehab center, but they did nothing for me.
I finally got out of there and back to the hospital to do rehab. In two weeks, I was able to stand at the parallel bars and sit in this wheelchair and push up. And then they started walking me, and it was amazing because I hadn't walked in ninety-something days. I got off-balance and never could get the strength. I would walk with a walker and then I would get tired. Like right now, I still get tired fast, I still don't have no balance, still can't taste every now and then, still can't smell every now and then.
I know there's a God 'cause it's a miracle that I am here. The guy's son who does the dialysis tell me, "Mr. Frank, you're a walking miracle." I say, "What are you talking about?" He say, "Frankie, everyone who
was on that floor that had COVID, all of them died but you." And he say, "I know there is a God, you blessed." Then Dr. V., the heart doctor, say, "Man, we really thought you was going to die." Dr. S., "Man, we really thought you was going to die." You know, it's a bad feeling when everybody coming to you, telling you that they really thought you was going to die. And they look at you, "Man, Frank!" and you don't remember. The doctor told me maybe it's good I don't remember. You know? And I'll be asking my wife, "What happened?" And she'll be telling me, and I don't remember. He said, "That's a part of your life that you will never be able to get back." That's fine, I'm here now. I don't wish this on nobody, man.
Emma, Arizona
Migrant Farmworker—February 2021

Our farmworker population start their days at 2:00 a.m., sometimes earlier. Approximately 15,000 to 20,000 of them cross every day, and the lines on the border can be two or three hours long. They leave early so they can make it here in time to get on the bus and be taken to the fields where they harvest the fruits and vegetables that America eats. This area around Yuma is called "America's Salad Bowl." Our organization provides services to our population, including immigration, housing, parenting, chronic disease prevention, and behavioral health. We're always very busy, so when we started hearing the news that this virus was impacting China and how bad it was, we didn't have a lot of time to think about it. We have a small, rural life, so you don't think a lot about whether something international will hit here. You don't think about how interconnected you are in reference to it. Then at the end of January, we had three cases. It was still not a pandemic at that point, and it was just three cases, so we were thinking, Okay, so three cases. We continued business as usual, no additional precautions, just basic hygiene and all that. When the governor issued a shelter-in-place order, we realized this was serious. Shops started closing and people were running around and piling up food and toilet paper.
After our agricultural season ended, a lot of our farmworkers migrated to California, particularly Salinas, San Joaquin, Santa Maria. Then we started hearing about the pandemic hitting them over there, and even some deaths. One man died in a hotel room by himself. The family knew he was very sick. Nobody was visiting him or giving him food or anything, according to the family. The only contact they had was just through the phone, and all of a sudden, he stopped answering. That's how they realized he had died.
During the stay-at-home order, I had a lot of thinking to do about our office here in Yuma. We have thirty employees, and it's important for personal and cultural issues to have direct, one-on-one contact with the individuals we serve. After the two weeks of stay-at-home, we opened the office back up. My husband used to work at the Health Department's emergency preparedness program and helped us understand the precautions we needed to take. We invested a lot of money in plastic safety barriers and hygiene equipment and products, and we had the offices fumigated every two weeks to sanitize them.
Then there was the question of whether to open the doors or lock them and make people knock. But I felt badly for the elderly or the farmworkers who just needed a form to be read or translated or just basic services like that. So I decided that we were going to have to take a risk and open the doors and do whatever we could and pray to God. We were going to face the threats and fight them because we could not be paralyzed; we have to continue serving our population. So we opened the doors. We let people in just two at a time or one at a time to keep as safe an environment for them and for us as possible.
When the agricultural season started back up again in October, the owners of the farms required the workers to wear masks and did temperature checks, but the buses were loaded just the same as before, everyone crowded in. We did two or three campaigns where we went to meet the loading area for the buses at three o'clock in the morning. We provided tote bags with masks, information, gloves, and everything. Our staff was wearing their gowns and PPE, like they were in a hospital. They were there, facing their fears, because what else could we do? One time we gave out about one thousand bags between 3:00 a.m. and 4:30 a.m.
At some point in the pandemic, we were ground zero in the world for the number of cases. The harvest season and the pandemic season collided. Many of the migrants were sick, but they wouldn't say anything. And a lot of them were young, between eighteen and thirty-six, and didn't show symptoms. Migrant workers don't get fringe benefits or sick leave or anything like that, so a lot of them, especially the H-2A temporary workers, didn't want to be quarantined for two or three weeks. So the sick workers wouldn't say anything and then the whole crew would get sick, but they would not say anything. The employers wouldn't say anything either. They wouldn't want the testing to be done for the workers and the workers wouldn't want to be tested, and so there was like this kind of silent agreement. "Don't ask, don't tell, because we need you and you need us." That is what I have been hearing.
Donna, Georgia
Senior Living Community Executive—July 2021
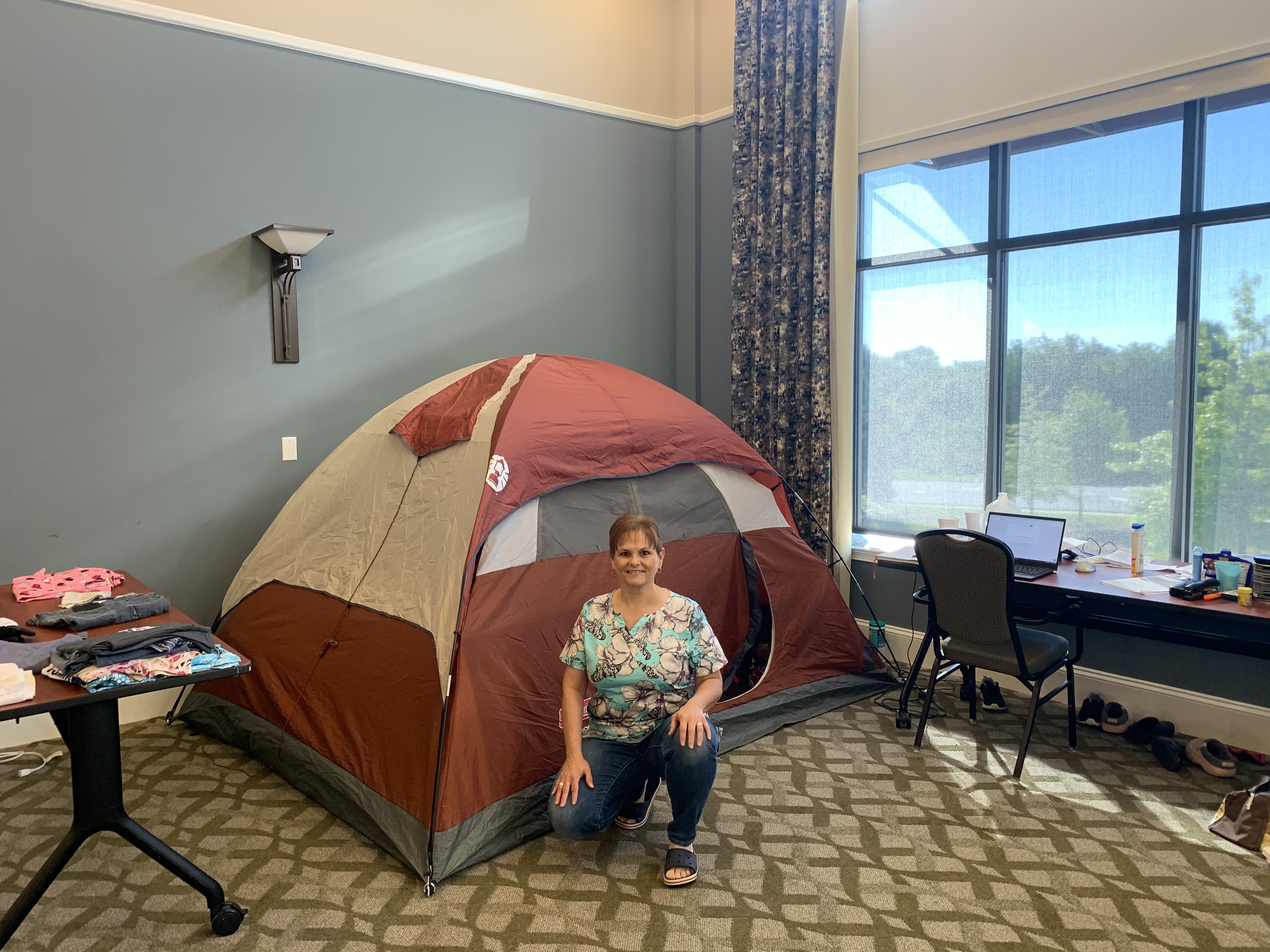
The coronavirus came to our campus on March 13. It was one employee and we sent them home. I then went to my boss, the CEO of our company, and said, "Our best strategy right now is to lock in. We'll ask employees to volunteer to live on campus and we'll reward them. And we will just live on campus with our members. It'll be over in two weeks, four weeks max." He never blinked. He was behind me 100 percent.
We didn't call it "lock out." We "locked in" with our members and we kept the world out. We kept coronavirus out. The gate was literally locked, and the only thing that came in and out of that gate was food deliveries, Amazon packages, and Instacart.
I asked for volunteers from our employee body, and sixty people raised their hands immediately.
They included our director of accounting, our moving coordinator, servers, housekeepers, maintenance, security. I took any volunteer who raised their hand. Ended up being seventy-five. The next step was figuring out where people were going to sleep, how we were going to feed employees, and how we were going to keep the operations of our 500-member community running with a staff of seventy-five instead of 300.
Some of the employees lived in model rooms, some lived in rooms on air mattresses, and some people, like me, lived in our health center, with memory care and skilled nursing. I lived in a tent in the community hall.
We left our titles at the door and we all took on different roles, whatever we needed to do to take care of members. Everybody at mealtime became someone that delivered meals. Everyone became someone who would disinfect our common areas. Everyone became whatever we needed them to be in the moment. I don't even know that some of my employees that I was serving with knew I was the COO. They just knew I was that girl that came and made French toast on Sunday mornings and vacuumed the hallways and helped do laundry. It didn't matter because it was all of us together, fighting a common enemy called COVID.
Each day, I would crawl out of my tent, put on my scrubs and ball cap, and go down to see who needed help with breakfast. I might be feeding a member, I might be cooking in the kitchen, I might be just engaging with members around a game of cards or a board game, or painting nails or giving a haircut. By the time breakfast was over, it was already lunchtime, and we were making sure that everybody was eating and getting their meals. Days were filled with making sure our households were clean, members' rooms were clean, laundry was done for everyone, and everyone received their medications. And spending time together, like sitting outside in the courtyard, soaking up the sun, talking and visiting. We did things to keep people entertained, too, like Zoom karaoke. They got such a hoot out of hearing me sing not well.
We were working twelve, fourteen, sixteen hours a day, doing what was needed and trying to keep everyone's spirits up. It was constant motion. I will admit that sometimes it was nice to retreat to my tent and just turn off the device and just be. I have an Energizer Bunny in my body, so it wasn't so much physically exhausting as much as just mentally exhausting. Retreating to my tent and just being by myself was a relief for me.
Two weeks went by and the coronavirus was a hot-fire mess in Georgia. Then four weeks. I got everyone together and said, "If you need to go home, you can. You did what I asked you to do. You committed for four weeks. But I still need you." That's the hardest thing I've ever had to do as a leader, to say, "You have given me what you promised, but I need more." And every time I did that, they would say, "You can count on me." And that's not about me, it's about what we do here. It's about our mission of loving and serving members. We make a promise to them that they never have to leave, that we will move them through the continuum of care as they progress in age, and that we will always take care of them.
This was a wonderful example of seeing people living our mission in action. It was about living it to the extreme. And it was a beautiful thing. Our employees talk about our members as their second family. We got to live that; we got to see it in action.
Employees made a commitment to leave their own families during this crisis so they could take care of the members of their second family. We have one director of nursing who has six kids, a husband, and her mom who lives with them. She talked to her family, and she said, "I feel like I need to do this." And the family said, "Don't worry about us. You go and do this and we will take care of home." I've got a picture of her standing in a window, looking at her family two stories down, waving up at the window. That's powerful commitment.
Growing up, my father was a soldier who went to Vietnam twice. You know, I was watching my father go off and hoping he would come back. With COVID, we knew we could lose members. If we didn't do extreme things like locking in, we could lose members, and we weren't willing to do that. That's what I learned from my father about mission and commitment.
We locked in for seventy-five days. When we did leave, it was because we had the processes in place, the PPE and testing in place, that we needed to make sure we could take care of our members and employees. But it was so interesting on that last day when everyone was leaving, and their families were meeting them in the parking lot. They all hung out in the parking lot talking, like they didn't quite know how to leave. They were a big family of seventy-three sisters and two brothers, needing to leave each other so they could be with their own families.
I was remembering that the other day when we finally were able to open up to family visits for our members. They had not seen their families in person, to be able to touch and hug each other, for over a year. Our staff, because they remember how emotional they were after the seventy-five days, were standing by the doors, crying, while the families were reuniting in the rooms. They knew.
We all walked away changed. You can't go through something like that and not be changed.
Michael, Texas
Bar Owner—January 2021

Bars are places that people rely on in disasters. We're community hubs, a place where people go to be able to contextualize what's going on. So even people who you might not see in a bar regularly, you'll see them in times of crisis because it's a place to get news, it's a place to get out of your house, and it's a place to be around people in your neighborhood or community and reassure yourself that there's other people like you. That things are going to be okay. This particular disaster, though, was one that featured humans gathering as the disaster.
When we had to shut down, we wanted to find a way to be able to serve our clientele. We have a community of people that rely on us to be there for them for whatever reason they need us.
People don't go to bars because they want to get drunk. You can get drunk anywhere. People go to bars because of the basic human need to connect. Given the way modern society is going, there's more and more separation and less and less connection. As grocery stores have gone from local shops to big-box stores, there isn't anyone there to talk with anymore. Same with coffee shops. And now that everything is automated and delivered, you can sit in your home and order everything you need and have every interaction through a computer.
We were very cognizant of the fact that the people that needed us as bartenders were still going to need us, and probably more because they were stuck at home, so whatever drove them out of their house in the first place, that hadn't gone away. And more than that, their social outlet was gone; their community gathering outlet was gone.
We started livestreaming from the bar. We went on every night for an hour, and we did all kinds of crazy things, like we sang karaoke for them, hosted trivia nights, and sometimes made cocktails. I called it a virtual bar, and we were as interactive as possible with people. Sometimes we had guests come on from other places in the country. We ended up building a really, really strong following. Basically, virtual bar clientele would sit at home and have a beer, or they'd have a drink of their own, and they would come and talk to us and they would watch us do silly stuff. We put out a tip jar that they could put money in for the staff. It was surprisingly powerful.
That lasted for a while until Texas reopened again, very early and very unwisely. At the time, we were getting towards the end of whatever resources we had, so we tried to open as safely as possible. That lasted for a couple of weeks until one of my bartenders got COVID. Then I was furious. Furious that we'd been put in the position of even trying to let people in our place. And so, out of pique, I recorded a video that was basically addressed to Greg Abbott, the governor of Texas. It was a plea from a bar in a pandemic. It ended up getting something like half a million views on social media. What a lot of people didn't realize was that bars were excluded from a lot of the aid being offered to small businesses during the pandemic. We were placed in a position of needing to open as soon as we were allowed to, even if it was unwise.
Pretty much right after my video, Texas closed down again because there was a big spike in cases. It was a big spike at the time, but compared to where we are now, it was nothing. That big spike that closed Texas down in July was a fraction of where we are now.
Mike, Florida
Doctor—January 2021
We have knowledge we learned based on our experiences in past pandemics. Yet, over the last year, we've acted like we learned nothing. That's very disheartening. We have had a lack of direction, and that's been very frustrating. They say that tough times bring out the best in people. It also brings out the worst in people. I have seen benevolence and kindness that was just phenomenal. And I have seen selfishness and self-centeredness that I would never have expected. It's really been an eye-opening experience.
My grandmother used to say, "I've been alive long enough that I have a right to say what I believe, especially if it's true." I'm not even close to her age, but that being said, I also feel that I've been around long enough, and especially around the medical field long enough, more than thirty-five years, that I can be open and honest.
Over the last year, I've become extremely disappointed with people, from leadership all the way down. I've seen political leaders come out and say, "The doctors and the medical experts say this, but I'm going to do what I want to do." And they're supposed to be our leaders. When people say, "I'm not going to follow guidelines because it's an infringement on my rights," I want to ask, "At what point does it become not all about you but all about everybody else and all about society?" Rather than people uniting with a focused approach, which would have led to a lot less suffering and death for many people, many leaders took such a selfish and self-centered approach that it made a bad situation terrible.
And I'll be honest, I would never have foreseen this happening. Previously, I thought that if we had a worldwide pandemic and we knew it and we saw it daily, that we would take the right approach, follow the high road, a consistent approach. We have done none of that.
I work as a hospitalist and do critical care medicine as well as palliative care work. In the Florida panhandle, our COVID hospitalization numbers have been climbing rapidly. From the beginning in March through November, I would have twelve to fifteen patients to work with each shift, with somewhere between two to four COVID patients. Occasionally, I had up to eighteen patients, but that would be a heavy load. On my shift a week and a half ago, I had twenty-six patients, fourteen of which had COVID. COVID-positive patients take about 50 percent more time. So taking care of twenty-six patients was actually like taking care of thirty-nine regular patients. Four of those patients were in the ICU on mechanical ventilators, which takes even more time.
I truly try to provide the best care I can for each patient, but at some point, it's like something's got to give. That is very disheartening to the doctors and nurses and other members of the medical team because we try to give our all, but unfortunately, it doesn't always work. I've taken care of hundreds of patients with this disease, and I've seen dozens and dozens die from it. Yesterday, more than 4,000 people died from COVID nationally. Many of those dying are young, and even more are dying alone.
It's frustrating when the emergency room is packed with COVID patients, the ambulance bays are packed with COVID patients, and we have no ICU beds available for our critically ill patients. I had a patient come in who was not COVID positive, but he was bleeding out from the bottom, terribly, and he had dropped his blood count by two-thirds.
When a COVID patient died, we cleaned the room and then put this guy in there, but he was the only non-COVID patient in the entire ICU. We have other patients coming in who need ICU beds, like patients with acute strokes and severe heart failure. When these patients come in and the hospital tells them, "We don't have any beds, you've got to go to another hospital," that means more time before they're admitted. As they say, every second is brain tissue in a stroke; every second is heart muscle in a heart attack. And we're having to divert these patients because there's no room. And if we can fit them in the hospital but not in the ICU, then they are put on other floors without the equipment and staffing needed to give them the proper care.
I started during the HIV days, so I've been doing this a long time. Now, when I get home after working up to sixteen hours instead of what is supposed to be a twelve-hour shift, I just try to close my eyes, sleep, and let it go. Because I know that I have to go back tomorrow and do it again. 
About the Author
Michelle Fishburne is a full-time digital nomad, splitting her time between her 2006 motorhome, Airbnbs, and the occasional housesitting gig.
Public Health in the US and Global South is a collection of interdisciplinary, multimedia publications examining the relationship between public health and specific geographies—both real and imagined—in and across the US and Global South. These essays raise questions about the origin, replication, and entrenchment of health disparities; the ways that race and gender shape and are shaped by health policy; and the inseparable connection between health justice and health advocacy.
Beginning in 2022, the series expands to include 1000-word blog posts, as well as longer commentaries, essays, articles and media productions that address the public health and political implications of the COVID-19 pandemic from multiple perspectives. The series editor for Public Health in the US and Global South is Mary E. Frederickson.
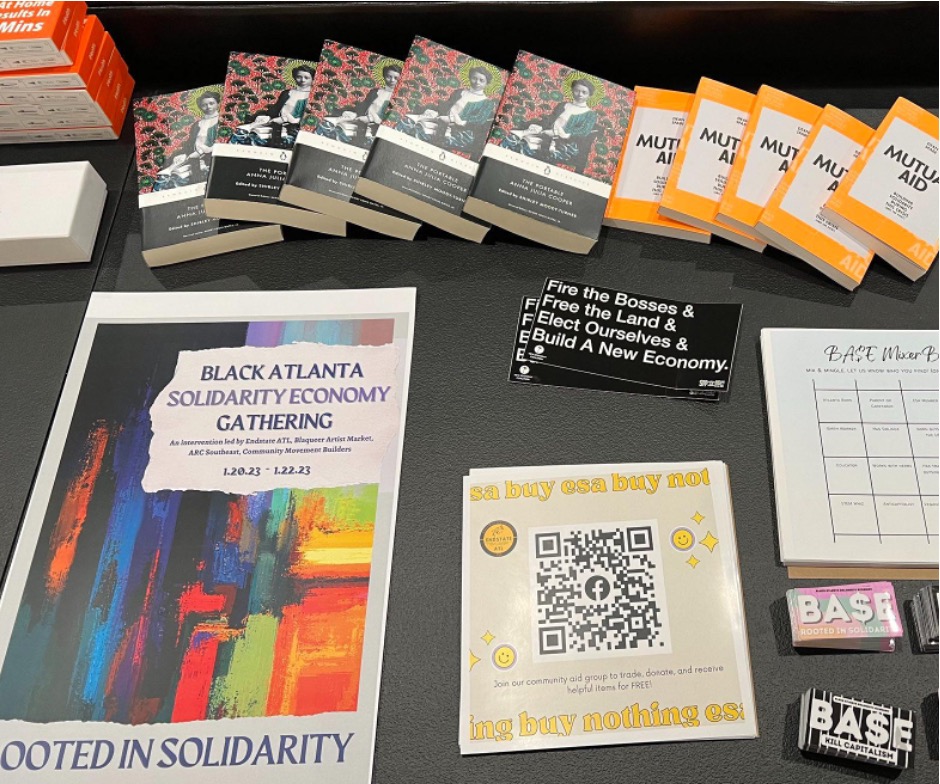
In May of 2023, when the World Health Organization downgraded the coronavirus emergency from a global health pandemic to an "ongoing health crisis," the shift made sense in many ways. Most developed nations have made vaccines available for over two years. Shutdowns and enforced quarantines ended, even in holdout nations. The WHO's announcement signaled that other countries, including the United States, would follow suit if they had not already. This move, however, will have material consequences for grassroots charitable organizations across the US. Endstate ATL (ESA), a group I have worked with since 2021, is one of many non-profit groups that will be affected.
In Georgia, the COVID state of emergency officially ended in May 2022, even as it remained in place at the national level. This allowed organizations like ESA to continue our mutual aid work. But when the US announced the end of the Federal COVID-19 Public Health Emergency (PHE) Declaration on May 11, 2023, enhancements to public assistance and social safety net programs ceased. From this point on, groups like ESA once again will have to jump through multiple bureaucratic hoops to obtain the funding necessary to provide care.
Following the global outbreak of COVID in 2020 many governments created temporary measures to extend aid to vulnerable populations. In the US, these included extensions of unemployment benefits, a moratorium on student loan interest and payments, no-cost COVID testing and vaccinations, Medicare flexibility, and opportunities to provide nontaxable disaster relief funds. The national government also released relief funds to individual state governments, although often these funds did not reach the people who needed them.1Rebecca Riess and Devon M. Sayers, "Alabama Governor Signs Bill to Use Covid-19 Relief Funds to Build Prisons," CNN, October 1, 2021, https://www.cnn.com/2021/10/01/politics/alabama-covid-relief-prison-bills-signed-governor-kay-ivey/index.html. Despite the uneven distribution of aid, many people, specifically children and elders, moved above the poverty line thanks to COVID assistance.2John Creamer, "Supplemental Poverty Measure That Accounts for Additional Government Benefits Lowest on Record at 7.8%," Census, September 13, 2022, https://www.census.gov/library/stories/2022/09/government-assistance-lifts-millions-out-of-poverty.html.

The flexibility surrounding nontaxable disaster relief funds eased mutual aid work. Mutual aid has a long history in the US and Global South, and the onset of the COVID-19 pandemic witnessed an outpouring of community solidarity towards those in need. Mutual aid stands apart from other charity models because of its non-hierachal emphasis on mutualism rather than models that maintain divisions between givers and receivers. Mutual aid is rooted in reciprocity.
Endstate ATL took advantage of these temporary measures for the betterment and aid of our community members. Rooted in southwest Atlanta with a Black queer feminist politic, ESA's work aims to reach those most marginalized through community building, political education, and mutual aid. Through our Black Power Fund, which pays up to three months' worth of utility bills for Black queer households, and our Pack Provides Programs, which provide household supplies, COVID PPE, and infant essentials including formula, clothing, and sanitary products to caregivers of young children, we seek to step in where the state fails to provide support.
Mutual aid allows organizations to provide immediate care and relief to individuals in need without imposing the bureaucratic processes that often keep aid beyond reach. Under a state of emergency, disaster relief payments are not taxable. As such, ESA, and other groups like it, were able to provide direct aid through a less convoluted system of reporting and disbursement. This allowed us to move funds directly and rapidly to people in need and has been crucial to our ability to substantively support people in a timely way. ESA has covered bills for ten households in the past year, as well as covered a year of utilities for the BARRED Business house, which provides stable, community-owned housing for people recently released from prison. We have been able to report these funds as disaster relief.3"Mutual Aid Legal ToolKit," Sustainable Economies Law Center, Accessed June 22, 2023, https://www.theselc.org/mutual_aid_toolkit.








The efforts of mutual aid groups helped supplement aid where state and local leadership failed. Georgia governor Brian Kemp refused to take the COVID-19 pandemic seriously. In 2020, Georgia was the first state in the nation to relax quarantine restrictions, even as Kiesha Lance Bottoms, the mayor of Atlanta, sought to retain many protective measures. Initial reporting that the virus would largely impact the elderly and immunocompromised, combined with anti-fear government propaganda, engendered a sense of invincibility and an attitude of disregard among many Georgians. As of 2021, Georgia had one of the highest COVID mortality rates in the US, and those most impacted were poor, working class, and people of color.4"COVID-19 Mortality by State," CDC, Accessed June 22, 2023, https://www.cdc.gov/nchs/pressroom/sosmap/covid19_mortality_final/COVID19.htm. The refusal of Governor Kemp to implement mandated social distancing or mask requirements, even before vaccines were available, left the entire state population vulnerable to infection. The consequences were devastating, with thousands of unnecessary deaths and debilitating outcomes for those suffering from long COVID.
Pandemic relief payments meant to alleviate the burden of rising interest rates were out of reach for marginalized Georgians. In order to receive national stimulus checks and Kemp's own "special tax credit," individuals needed to have filed and paid taxes for the preceding two years, a barrier that left people who were unemployed or homeless without access to relief.5"Gov. Kemp Announces First Round of This Year's Special Tax Refund," Department of Revenue, May 1, 2023, https://dor.georgia.gov/press-releases/2023-05-01/gov-kemp-announces-first-round-years-special-tax-refund#:~:text=Single%20filers%20and%20married%20individuals,a%20maximum%20refund%20of%20%24500.

In response to the pandemic, groups emerged such as Bed Stuy Strong, based in Brooklyn, which created a robust grocery delivery system by first relying on the resources at their disposal before evolving into a program that benefited thousands.6Haritha Kumar, "Four Key Takeaways from Mutual Aid Organizing During the COVID-19 Pandemic," Georgetown University Beeckcenter, October 4, 2022, https://beeckcenter.georgetown.edu/four-key-takeaways-from-mutual-aid-organizing-during-the-covid-19-pandemic/. Georgia has similar organizations. Community Movement Builders developed stabilization programs that include rent/mortgage payments as well as groceries in their efforts to impede the gentrification of southwest Atlanta, and Food4Lives a non-profit started by Georgia Tech and Emory students provides food and supplies for the unhoused in the greater Atlanta area.7Katie Burkholder, "Housing as a Human Right: Community Movement Builders Organize Against Gentrification," Georgia Voice, April 21, 2022, https://thegavoice.com/today-in-gay-atlanta/housing-as-a-human-right-community-movement-builders-organize-against-gentrification/; "Who are We?" Food4Lives, Accessed June 22, 2023, https://food4lives.org/about.html. Both organizations preceded the pandemic, but their work became much more indispensable in its wake.
The increase in groups doing this aid work was significant, especially in red states where Republican leadership champions laissez-faire government structures for almost everything but reproductive health, policing, and surveillance. Pandemic or no pandemic, people need help. However, smaller aid groups face difficulties in keeping the work going. ESA has primarily been funded by grants, a funding model that is not easily sustainable. According to one of our members, "A significant struggle we've faced since the end of the COVID-19 pandemic is the philanthropic and public perception that the conditions for folks have changed enough that mutual aid is not necessary even as we continue to field a significant number of requests." Further, all members participate on a volunteer basis, spending much of our time otherwise as graduate students, teachers, doulas, herbalists, and nonprofit workers. Over the last two years, many of us have faced our own destabilizing events, financial uncertainty, bouts of COVID, and family loss. The ability of small groups to come together and push to make a difference in their communities—despite personal difficulties and decreasing assistance from governing bodies—should inspire more activism. But the question remains, how can we continue this work when governmental policies have resumed restricting social safety nets while offering few, if any, alternatives?
Changing policy is one problem organizers face, burnout is another. Studies have suggested that we approach "burnout as a part of activism and as influenced by the organizational context, rather than as something that individual activists experience outside of activism."8Maria Fernandes-Jesus et al., "More Than a COVID-19 Response: Sustaining Mutual Aid Groups During and Beyond the Pandemic," Frontiers in Psychology 12 716202, October 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8563598/. However, as young Black people organizing in the South, my colleagues and I experience burnout from many directions. We deal with the stress of everyday life, as well as the difficulty of doing our solidarity work, with constant reminders from government leadership that our goals are at odds with theirs.
With the COVID state of emergency ending in the US, aid provided by organizations such as Endstate ATL becomes taxable, dramatically altering the way funds can be mobilized, as well as the process that recipients must go through to receive support. Charitable tax deductions are reserved for individuals and corporations who donate money to qualified charities.9Up until December 2021, entities meeting these requirements were able to claim as much as 100% of their AGI in charitable tax write offs. "CARES Act Charitable Benefits Not Extended For 2022," Stanford Giving, March 14, 2022, https://giving.stanford.edu/stories/cares-act-not-extended-for-2022/. Because ESA puts money "directly" in the hands of marginalized people, such direct contributions to individuals are not tax-exempt. The COVID state of emergency allowed groups like ESA to move funds to individuals more freely—on an emergency basis. The end of the state of emergency means we must restructure our aid programs. The beautiful thing about mutual aid is that even if one group burns out, another group can and likely will step up right behind to fill the gap. In this way, the work continues. We never stop.
About the Author
Ra'Niqua Lee writes to share her particular visions of love and the South. She earned an MFA in fiction from Georgia State University, and she is currently at Emory pursuing a PhD in late nineteenth/early twentieth century African American literature with a focus on spatial and Black queer feminist theories. Her fiction has appeared or is forthcoming in Cream City Review, SmokeLong Quarterly, Indiana Review, Passages North, Best of the Net 2023, Best Small Fictions 2023, and elsewhere. In 2021, the Georgia Writers Association awarded her the John Lewis Writing Grant for fiction. Her flash collection For What Ails You is forthcoming from ELJ Editions.
Acknowledgments
Many thanks to my colleagues. Without their collaborative support, I would not be able to do this work: Julian Rose, Britni Ruff, Christina Foster, Michelle, Jovan Julien, and extra thanks to Hugh Hunter for his early edits.
Public Health in the US and Global South is a collection of interdisciplinary, multimedia publications examining the relationship between public health and specific geographies—both real and imagined—in and across the US and Global South. These essays raise questions about the origin, replication, and entrenchment of health disparities; the ways that race and gender shape and are shaped by health policy; and the inseparable connection between health justice and health advocacy.
Beginning in 2022, the series expands to include 1000-word blog posts, as well as longer commentaries, essays, articles and media productions that address the public health and political implications of the COVID-19 pandemic from multiple perspectives. The series editor for Public Health in the US and Global South is Mary E. Frederickson.
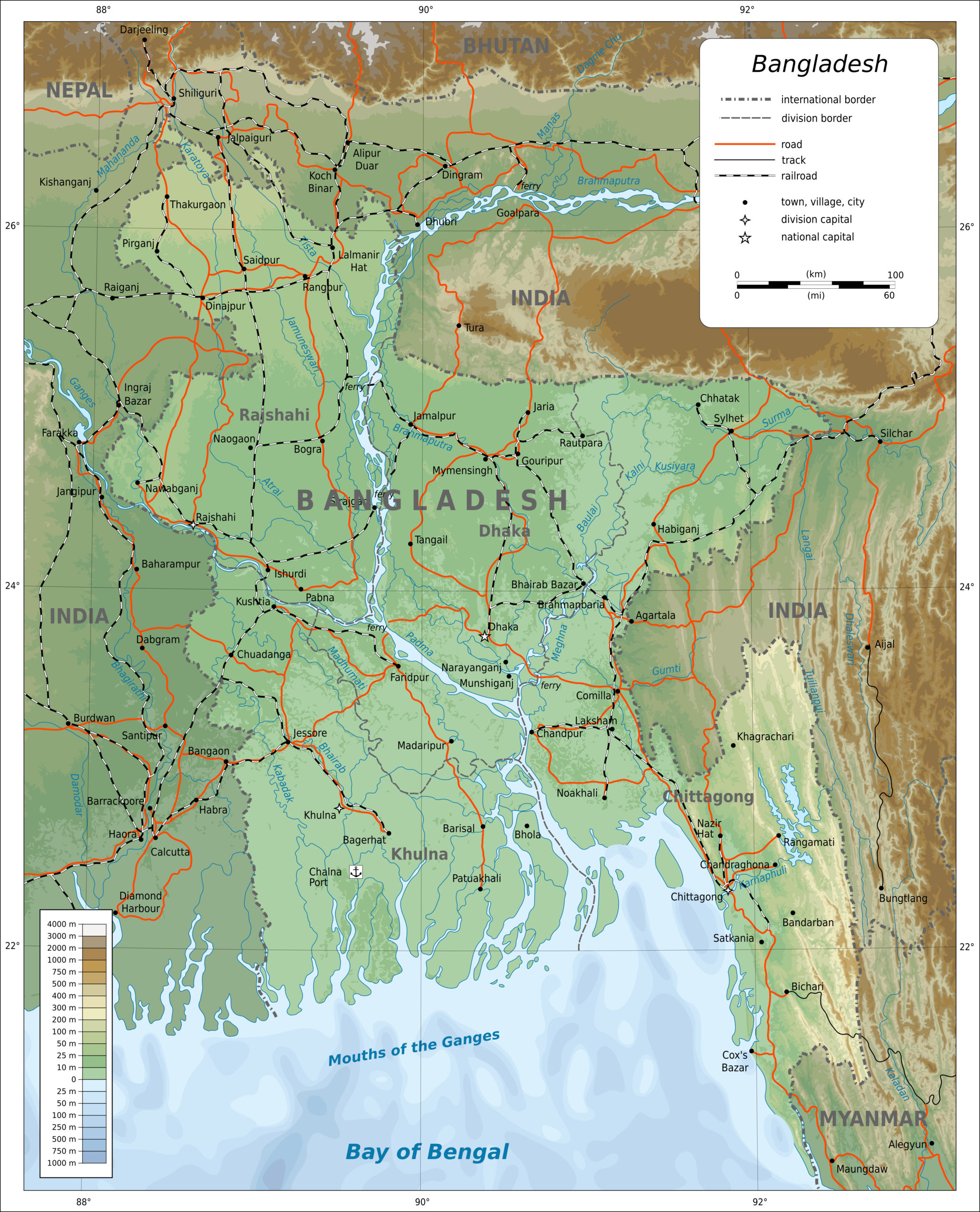
As the world moves into its fourth year since the advent of COVID-19, the pandemic remains a broad public health concern. It is necessary to teach Covid-appropriate behaviors and build public confidence in vaccines and boosters to address new strains of the virus. Across the globe, localized Covid pandemic response projects should complement conventional approaches to preparedness. Community Support Team Dhaka (CST Dhaka) and Community Support Team Cox's Bazar (CST Cox's Bazar) are two projects implemented by the health program of BRAC, a Bangladesh-based NGO.
Bangladesh, the eighth-most populous country in the world (169.4 million people), is a developing country located in South Asia with a 2021 gross domestic product per capita of $2,458. The country has achieved significant progress in reducing maternal, infant, and child mortality rates, decreasing malnutrition, improving immunization coverage, and eliminating infectious diseases like polio. However, it faces emerging health challenges, including the growing burden of noncommunicable diseases, heightened vulnerability to disasters and environmental hazards, and the threat of health emergencies during disease outbreaks such as COVID-19. Bangladesh's health services are centralized and urban-centric.1There are only 1.1 doctors per 10,000 people in rural populations in Bangladesh, while there are 18.2 doctors per 10,000 people in urban areas. Taufique Joarder, Lai B. Rawal, et al, "Retaining Doctors in Rural Bangladesh: A Policy Analysis," International journal of Health Policy and Management 7, no. 9 (2018): 847–858. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6186485/. The country also faces shortages of well-equipped healthcare facilities and healthcare workers. The health financing system in Bangladesh suffers from a lack of adequate funding, absence of appropriate health insurance, and a large dependence (74%) on out-of-pocket payments.
BRAC, founded in 1972, is the largest non-governmental organization in Bangladesh involved in a variety of sectors including public health, education, microfinance, and livelihood support. It currently employs over 100,000 people across Bangladesh and ten countries. Its Health, Nutrition, and Population Programme (HNPP) has been a global leader in developing and scaling up locally-based health worker programs for the rural population. With support from the Foreign, Commonwealth & Development Office (FCDO), the World Bank, and the United Nations Population Fund (UNFPA), the organization implemented two COVID-19 response projects in Dhaka and Cox's Bazar (two of the high-risk districts identified by the World Health Organization after analyzing infection rates in different districts of Bangladesh). BRAC initiated several creative approaches in these locations to tackle the spread of COVID-19 at the height of the pandemic.
"Miking" in Local Dialects

Playing health messages through mobile loudspeakers (locally known as miking) has been around for decades. After the initial round of miking in Cox's Bazar, however, the volunteers and area managers heard from local representatives that the messages in mainstream Bengali were not effectively reaching the people. Here, the Chatgaya/Chittaingya dialect is the primary oral language. Subsequently, the Cox's Bazar project engaged a local voiceover specialist to develop messages in Chittagonian dialect which enhanced the effectiveness of the 849 miking sessions conducted in the region, substantially improving the local population's understanding about vaccination.
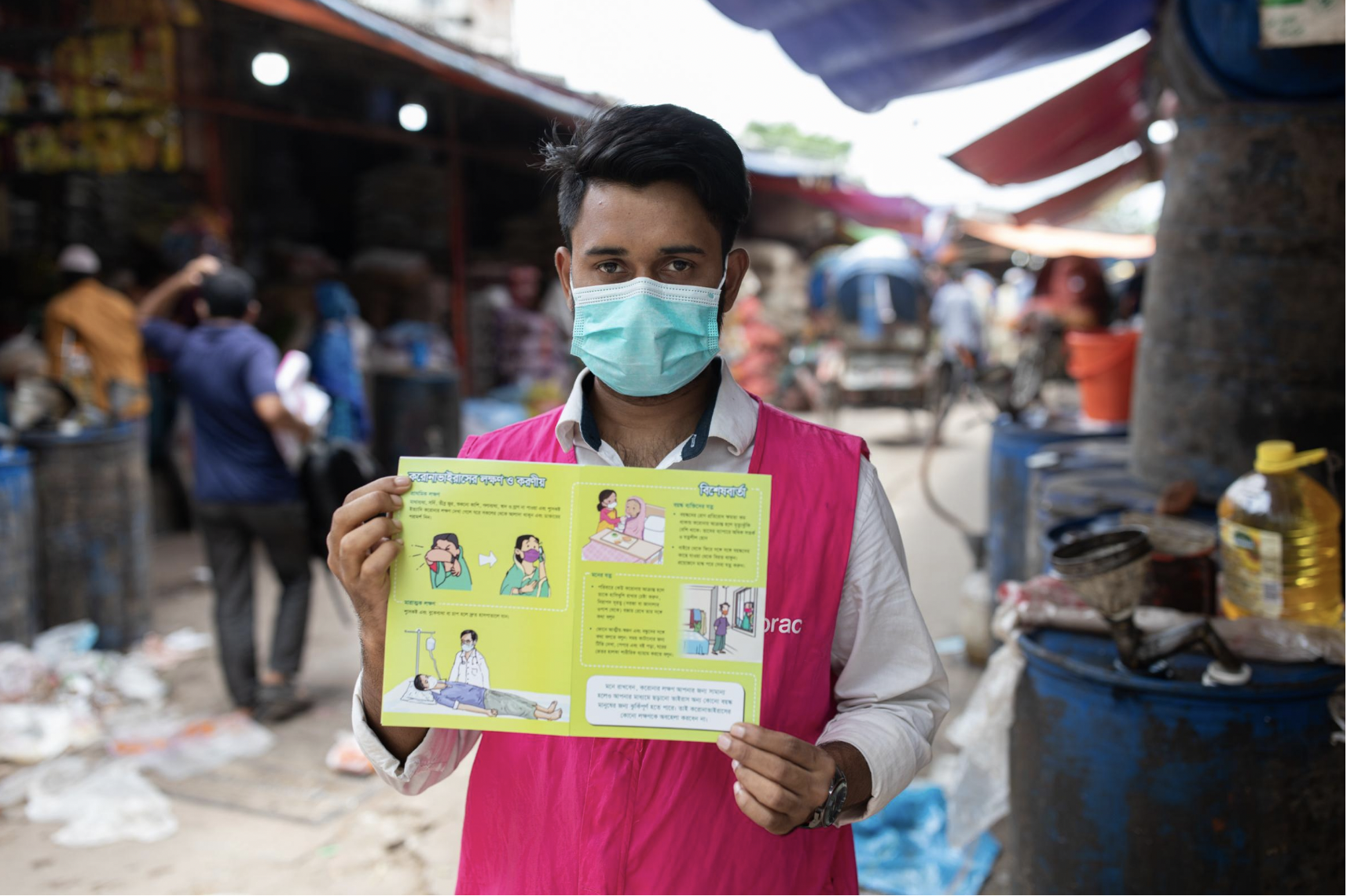
Info Cards
A common request received by the field staff (community health workers, volunteers, and area managers) was for comprehensive materials to complement the messages disseminated verbally. In addition to the usual posters, stickers, and leaflets, BRAC designed tri-fold cards with detailed information on vaccination, handwashing, mask wearing and disposal, and instructions about taking care of people with comorbidities. Info cards were distributed to local change-agents such as market committee members or transport hub leaders to help sustain best practices. The cards garnered a positive response from the public.
Collaboration with Sisimpur
As schools in Bangladesh reopened after an eighteen-month shutdown, BRAC collaborated with Sisimpur—a local adaptation of children's television series Sesame Street—in creating an educational video about COVID-19 featuring the Sisimpur characters. Originally developed for the Dhaka project, this video ran on social media platforms and was shown at some three hundred schools. This intervention was entirely novel for many students and schools, and Sisimpur was also warmly received by parents and teachers. Unfortunately, this project began halfway through BRAC's wider Covid education initiatives, and needed more time and closer supervision.
Comics and Murals
Long perceived as reliable messengers in Bangladesh, local artists often translate crucial information into personable and understandable forms. Working with these artists, BRAC delivered COVID-19 information to schools in an engaging way. Renowned cartoonist Morshed Mishu developed wall murals in Dhaka and Cox's Bazar and 200,000 copies of a comic strip were distributed among schools and madrasas.






Faith Leaders' Endorsement
Faith leaders have addressed misinformation and influenced health behavior changes with a high degree of success. During the biggest Ebola outbreak in history, interfaith leaders were instrumental in delivering health messages in parts of West Africa that governments and NGOs could not reach. As credible sources of information, they worked actively on quashing rumors regarding Ebola and encouraged people to listen to government directives and the health workers.2A 2020 study by Afrobarometer revealed that across 34 countries in Africa, faith leaders are more widely trusted than any other public leaders. Brian Howard, "Religion in Africa: Tolerance and Trust in Leaders are High, but Many Would Allow Regulation of Religious Speech," Afrobarometer Dispatch no. 339 (2020), https://afrobarometer.org/sites/default/files/publications/Policy%20papers/ab_r7_dispatchno339_pap12_religion_in_africa.pdf. Early in the COVID-19 epidemic, BRAC teamed up with Islamic Foundation Bangladesh (IFB) and Bangladesh Baptist Church Fellowship (BBCF) to train their directors on best practices. Local representatives of UNICEF, who had previously engaged Muslim leaders in another health project, facilitated the IFB partnership. BRAC provided online training to IFB field supervisors and BBCF pastors via Zoom, addressing questions and rumors. This collaboration provided 3,400 faith leaders with awareness messaging, 860,000 reusable masks, and 350,000 leaflets.




Faith leaders and scholars such as Leor P. Sarkar (General Secretary of the BBCF), Gazi Sanaullah (Islamic scholar), and Pragyananda Bhikkhu (Assistant Director, Ramu Central Sima Bihar) endorsed preventive measures and appeared in short social media videos in support of wearing masks, maintaining social distance, washing hands, and taking vaccines.
While the Dhaka Community Support Team emphasized partnerships with selected faith-based organizations, Cox's Bazar sought to unite all the faith leaders from the intervention areas—Muslim, Buddhist, and Hindu—under one roof for knowledge sharing and collaboration. These meetings included a moderated session that provided equal opportunity to representatives of each religion to share the lessons they had learned. In Ramu, faith-based organizations overcame the silos between their work, meeting to formulate policies for combating the spread of vaccine misinformation. Volunteers working with faith-based groups increased both the reach and acceptance of the interventions.
Faith leader Reverend Leor P. Sarkar speaks on Covid,
Bangladesh. Translated from original Bengali.
Faith leader Gaji Sanaulla Rahmani speaks on Covid,
Bangladesh. Translated from original Bengali.
Interactive Popular Theater
BRAC's popular theater groups under its Social Empowerment and Legal Protection program (SELP), have performed about a wide range of topics such as gender equality, child marriage, violence against women, health, migration, and road safety across sixty-one districts since 1998. To raise COVID-19 awareness, the Cox's Bazar project organized 160 performances, despite dealing with some local challenges. For instance, the acceptance level of popular theatre was lower among the conservative Muslim population and the shows were more difficult to organize in hard-to-reach locations. Social distancing was more challenging when children made up the majority of the audience.

Findings from surveys and focus group discussions indicated increased awareness about COVID-19 symptoms, modes of transmission, and prevention measures (handwashing, mask wearing, social distancing) and vaccination across all intervention areas. Local knowledge about the existence of the virus and its spreadability increased.3Compared to the baseline, 26% more people knew that both hands need to be washed, 11% more people knew not to use a damp or damaged mask, whereas 7% more people knew not to wear the mask loosely. 8% more people reported knowing that the Covid-19 vaccine improves the body's immunity against the virus. School surveys revealed that 10% more students reported that face-to-face communication with the infected was the mode of transmission and almost 4% more knew it could be transmitted through coughing and sneezing. Encouraging accessible, engaging, and equitable approaches to public health communications has led to an increase in the uptake of COVID-19 preventive practices, as well as a reduction in barriers to vaccine confidence.
COVID-19 continues to pose a significant public health concern for many countries, like in India. While Bangladesh faces various health challenges and lacks adequate healthcare facilities and workforce, local NGOs like BRAC have played a significant role in addressing the pandemic's impact through introduction of localized initiatives like miking, info cards, Sisimpur PSAs, comics and murals, and faith leaders' endorsement to strengthen COVID-19 response. Such programs are essential in complementing conventional approaches to pandemic preparedness and mitigating the virus's spread. While these initiatives may be unique to Bangladesh, their successes can provide important lessons for other countries in terms of pandemic response and preparedness.
About the Author
Monzur Morshed Patwary is a public health practitioner with over eleven years of professional experience. As a senior program manager at BRAC, he has led several large-scale projects involving COVID-19 response, maternal and child health, and digitalization of training for community health workers. He has also collaborated with UN organizations and international donors such as USAID, FCDO, DANIDA, and GAC and helped mobilize high-value grants through project design and proposal development. Monzur represents Bangladesh on global platforms such as ParisWHO, Global Leadership Forum and HPAIR Harvard Conference. He completed the Hubert H. Humphrey Fellowship at Emory University-Rollins School of Public Health and is currently pursuing his professional affiliation at The Task Force for Global Health.
Public Health in the US and Global South is a collection of interdisciplinary, multimedia publications examining the relationship between public health and specific geographies—both real and imagined—in and across the US and Global South. These essays raise questions about the origin, replication, and entrenchment of health disparities; the ways that race and gender shape and are shaped by health policy; and the inseparable connection between health justice and health advocacy.
Beginning in 2022, the series expands to include 1000-word blog posts, as well as longer commentaries, essays, articles and media productions that address the public health and political implications of the COVID-19 pandemic from multiple perspectives. The series editor for Public Health in the US and Global South is Mary E. Frederickson.
Commentary
Multiple COVID-19 waves have left in their wake compelling evidence of long overlooked gaps in pandemic readiness and responsiveness. The primary lesson for the US public health and healthcare sectors is that this deep-rooted ignorance took a huge toll on their ability to contend with a novel, rapidly spreading, and lethal contagion. As historian Peter Burke recently noted: "Many vivid examples of the consequences of ignorance come from the history of diseases."1Peter Burke, Ignorance: A Global History (New Haven: Yale University Press, 2023), 189. COVID-19 is a current case in point. What was missed or mismanaged in the run up to the pandemic and during its catastrophic course will, if left unexamined and uncorrected, lead to enormous suffering and loss in additional public health crises. In this commentary, I want to elaborate on how institutionalized ignorance affected the Centers for Disease Control and Prevention's (CDC's) response and what can and should be done to learn from the agency's mistakes, with the goal of avoiding a repetition.

A thorough and fully transparent probe of CDC's recent history is warranted, one that scrutinizes "institutional obliviousness, under a succession of agency directors and programmatic leaders, to basic gaps in readiness and responsiveness that became glaringly obvious during the pandemic and contributed to numerous missteps in the US response to COVID-19."2Daniel Pollock, "COVID-19 Lessons in Ignorance," Southern Spaces, April 28, 2022, the first in a public health series covering the pandemic: https://southernspaces.ecdsdev.org/2022/covid-19-lessons-ignorance/. Far too much had to be cobbled together on the fly in early 2020 largely because of prior organizational neglect. And far too little has changed three years later, even as CDC moves ahead with its latest—to date, largely upper echelon—reorganization.3Centers for Disease Control and Prevention, "CDC Moving Forward Reorganization: A Notice by the Center for Disease Control," Federal Register 88, no. 29 (2023): 9290, https://www.federalregister.gov/documents/2023/02/13/2023-02929/cdc-moving-forward-reorganization.
Yes, SARS CoV-2 is a novel pathogen that spread rapidly, wreaked extraordinary devastation, and evolved quickly. Lots of impromptu learning about the virus and measures to contain or counter was necessary. However, pandemic warning signals abounded for years, and many assets CDC needed to function optimally in public health emergencies—as well as in non-pandemic times—were long overlooked or chronically under supported by virtue of the agency's own strategic planning, programmatic priority setting, and discretionary funding decisions. In surveillance and data science, for example, CDC did not fully mind and mend critically important gaps in electronic case reporting, immunization information systems, forecasting and outbreak analytics, and tools and dashboards for data visualization.
Certainly, factors largely beyond CDC's control had major impacts on the agency's performance. Besides the virus itself, CDC had to contend with (1) a coterie of federal government executives, most notably the 45th President, who failed to respond effectively and exerted unprecedented political interference; (2) a legacy of outbreak responses in the United States that are highly decentralized and contingent on a variety of situational circumstances; (3) longstanding constraints on CDC's public health authorities; and (4) chronic underfunding of public health programs at all levels of government. Each of these factors helps explain limitations, gaps, and shortcomings in the agency's performance. However, to leave the matter there would mean overlooking the impact of internal organizational factors that remain largely under CDC's control. Whether the agency has fully reckoned and responded to its internal problems is an open question that warrants much more attention.

"To be frank, we are responsible for some pretty dramatic, pretty public mistakes, from testing to data to communications," CDC Director Rochelle Walensky acknowledged in August 2022. However, the full CDC Scientific and Programmatic Review report that prompted Dr. Walensky's critique remains under wraps and not publicly available. Many months after the report was completed, all that CDC has published is a high-level summary and set of recommendations.4"CDC Moving Forward Summary Report," Centers for Disease Control and Prevention, Last reviewed September 1, 2022, https://www.cdc.gov/about/organization/cdc-moving-forward-summary-report.html. What was covered in the review, its methods and findings, and how conclusions were reached are shrouded in secrecy. Sequestering the report does not bode well for efforts to learn from CDC's COVID-19 experience and improve the agency's performance. Instead, CDC leaders have opted for a form of knowledge concealment that serves to perpetuate institutionalized ignorance.
For those of us who are deeply concerned about where the agency is headed, this is a fraught moment, yet organizational dysfunctions, mishaps, setbacks, and downturns are not necessarily points of no return. Learning from the COVID-19 pandemic and CDC's response to it can lead to changes that help revitalize the agency. Concealing the recent scientific and programmatic review report is not a good start along the path of organizational learning.

"Organizational learning," according to a leading researcher in the field and her colleagues, "is a process through which experience performing a task is converted into knowledge, which, in turn, changes the organization and affects its future performance."5Linda Argote, Sunkee Lee, and Jisoo Park, "Organizational Learning Processes and Outcomes: Major Findings and Future Research Directions," Management Science 67, no. 9 (2021): 5399–5429. The process should include gathering and moving information across organizational boundaries; eliciting and using multiple viewpoints; acknowledging hierarchies, policies, and practices that have not worked; and trying new approaches that have a higher likelihood of success. A prime example of an opportunity to learn from the COVID-19 experience is reckoning with how the agency organized, staffed, and operated its emergency response. From my perspective, the structure and process defects were profound and persistent, with the upshot that returns on the extraordinary time and effort so many CDC responders committed to their tasks fell well short of what would warrant use of all those precious resources. What purposes did the CDC response serve? Did the agency achieve those purposes? What was necessary to get the job done? Among the more specific questions about CDC's emergency operations is whether all the work involved with preparing, clearing, and presenting extensive PowerPoint slide decks in daily COVID-19 briefings was worthwhile. What were the benefits and at what cost?
Most of CDC's performance problems during the pandemic were the legacy of organizational neglect, not the exigencies of a novel corona virus or other external factors. The botched laboratory test rollout, flawed testing guidance, poorly prepared public health guidelines, confusing messaging, misguided mask recommendations, multiple data and analytic deficiencies, staffing shortfalls, and publication delays are traceable to assumptions widely held within the agency about institutional readiness coupled with longstanding inattentiveness by CDC directors and programmatic leaders to known or partially understood gaps. That CDC was not ready to go live sooner with a publicly facing, state-of-the art COVID-19 data display epitomizes what the agency had neglected. Instead, other data visualization websites, most notably Johns Hopkins University's dashboard, served as the go-to destinations for pandemic surveillance data. The reputational damage to CDC is severe and could have been avoided.
So much had to be launched or improvised by CDC in crisis mode because so much had been taken for granted or ignored for such a long time. Some additional examples from my own experience: When I joined the CDC response as Deputy Incident Manager for data and surveillance at the end of March 2020, I was surprised to learn that the agency had yet to introduce a process to enable secure data access and distribution of COVID-19 data sets to prospective data users who had been identity-proofed by the U.S. Department of Health and Human Services. Further, CDC had taken no steps to inventory and document relevant data sets and make provisions for sharing de-identified data with news organizations, one of which moved forward with a lawsuit to gain access to COVID-19 case data aggregated by CDC. The agency should have closed these basic gaps in data provisioning well before the pandemic, not during the throes of it. The only explanation of this blunder that I can think of is lack of forethought and follow through.

SARS CoV-2 is not the first viral respiratory pathogen to emerge and spread across country borders in the twenty-first century. While each international outbreak has presented a unique mixture of causes and consequences, they also have had much in common. That commonality places a premium on learning from each event and applying take-away lessons in a thoroughgoing way. What's ahead epidemiologically can surpass what's happened already in terms of complexity and magnitude, and that only heightens the stakes for CDC's organizational learning and pandemic preparedness.
While there are many pockets of CDC excellence, the organization, most notably because of its COVID-19 response, has taken multiple hits—some reflect ignorance about the agency's mission, operations, opportunities, and constraints but others are knowledgeable, on target, and of high consequence. There is much to do—and soon. We need to know more about CDC's performance gaps and shortcomings, and how to remedy them. To that end, instead of treating the full details of CDC's COVID-19 mistakes as a sequestered resource, it behooves CDC leaders to build on, transfer, and most importantly, act on what has been learned.6Jeffrey Pfeffer and Robert I. Sutton, The Knowing-doing Gap: How Smart Companies Turn Knowledge into Action (Cambridge, MA: Harvard Business School Press, 2000): 261. In the pandemic's wake, a much stronger commitment to organizational learning by CDC will provide the quickest and most effective solutions to the institutionalized ignorance that placed the public and the agency at risk.
About the Author
After completing the CDC's Epidemic Intelligence Service training program in 1986, Daniel Pollock worked as a medical epidemiologist at the agency for 35 years. Dr. Pollock led the CDC unit responsible for national surveillance of healthcare-associated infections from 2004–2021, and he served in CDC's COVID-19 emergency response in the spring of 2020 as the Deputy Incident Manager for data and surveillance.
Public Health in the US and Global South is a collection of interdisciplinary, multimedia publications examining the relationship between public health and specific geographies—both real and imagined—in and across the US and Global South. These essays raise questions about the origin, replication, and entrenchment of health disparities; the ways that race and gender shape and are shaped by health policy; and the inseparable connection between health justice and health advocacy.
Beginning in 2022, the series expands to include 1000-word blog posts, as well as longer commentaries, essays, articles and media productions that address the public health and political implications of the COVID-19 pandemic from multiple perspectives. The series editor for Public Health in the US and Global South is Mary E. Frederickson.
Commentary
As a public health professor at the University of Michigan, I've encountered opinions about the Covid vaccine in my own family that reflect mistrust and hesitancy. I can understand this.1Melissa Creary, "Bounded Justice and the Limits of Health Equity," Journal of Law, Medicine & Ethics 49, vol. 2 (2021): 241–256; Creary, "Legitimate Suffering: A Case of Belonging and Sickle Cell Trait in Brazil," BioSocieties 16 (2021): 492–513; Creary, "Biocultural Citizenship and Embodying Exceptionalism: Biopolitics for Sickle Cell Disease in Brazil," Social Science & Medicine 199 (2018): 123–131; Melissa Creary, Paul Fleming, Sheeba Pawar, and Amel Omari, "Leading with HEART: Working Toward Health Equity with Anti-Racist Teaching," The Pursuit, University of Michigan School of Public Health, April 29, 2021, https://sph.umich.edu/pursuit/2021posts/leading-with-heart.html; Creary, Paul Fleming, Trivellore Eachambadi Raghunathan, "The Impact of Race on Data." University of Michigan Population Healthy Podcast, February 16, 2021, https://sph.umich.edu/podcast/season3/the-impact-of-race-on-data.html; Creary and Anne Pollock, "How COVID-19 has highlighted racism as a health risk." King's College London Podcast, June 11, 2020, https://www.kcl.ac.uk/news/how-covid-19-has-exposed-racism-as-a-health-risk. Like many Black households in the US, my family had little reason to "trust the science," especially that produced during the presidency of Donald Trump, who consistently endorsed racist policies and spewed racist rhetoric.2Karen Grigsby Bates, "Is Trump Really That Racist?" NPR, October 21, 2020, https://www.npr.org/2020/10/19/925385389/is-trump-really-that-racist. While the public health response in the United States to COVID-19 was uneven across federal, state, and local entities, the narrative about disproportionate risk and mortality became apparent early and the public health establishment eventually sprang into action to make a case for health equity in the deployment of testing, prevention, and care.3Tasleem J. Padamsee, Robert M. Bond, Graham N. Dixon, et al, "Changes in COVID-19 Vaccine Hesitancy Among Black and White Individuals in the US," JAMA Network Open 5, no. 1 (2022), https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2788286. A survey published in January 2022, found that COVID-19 vaccine hesitancy had decreased more rapidly among Blacks than among whites since December 2020. Researchers found that Blacks "more rapidly came to believe that vaccines were necessary to protect themselves and their communities."
Even with these efforts, many of my family members initially could not be persuaded to take the vaccine. I was increasingly frustrated and wished they had more faith in science. Yet, even though I was vaccinated, I shared some of their concerns, and as I've written: "how can people who have never experienced equity be trusting of a supposedly new urgent call for equity when it comes to the vaccine?"4Fabiola Cineas, "Black and Latino Communities are Being Left Behind in the Vaccine Rollout," Vox, February 24, 2021, https://www.vox.com/22291047/black-latino-vaccine-race-chicago. If there were a culture that recognized a right to healthcare, would my family feel the same way? If we expected the state to have responsibility for our health and if we had a history of the public health system systematically and consistently providing preventative treatments and care, regardless of partisan politics, would it make a difference in vaccination rates in the present crisis?
In addition to studying health justice and equity in the United States, I have researched health policy development in Brazil. Segments of the Brazilian Black Movement in the 1990s, modeled to a significant extent on the 1960s US Civil Rights Movement, demanded the right to healthcare. Black participants in my Brazilian study deployed policy-based attempts to achieve full access to citizenship—most prominently as a right to health rights.5Creary, "Bounded Justice," 241–256. My work in Brazil explored how patients, non-governmental organizations, and the Brazilian government, at state and federal levels, have contributed to the discourse of sickle cell disease (SCD) as a black disease, despite a prevailing cultural ideology of racial mixture. Drawing on ethnography and oral histories from Rio de Janeiro, Salvador, Brasília, and Porto Alegre, this project charts the simultaneous constructions of race and science through SCD across Brazil. When I lived in Brazil in 2013, I was struck by just how much everyday people, within social movements and as part of civil societies, called on the Brazilian state to manage and provide healthcare access. With this in mind, I compare the public health systems in the United States and Brazil, the right to public health, and the COVID-19 vaccine.
The rollout of Covid vaccines in the United States was painfully slow. The Trump administration's Operation Warp Speed broke records in vaccine development in 2020, but floundered badly when it came to distributing immunizations in early 2021. President-elect Biden set the goal of deploying 100 million vaccinations in the first 100 days of his administration, pledging to streamline delivery throughout the nation. Shots went into arms and by mid-March 2021, a quarter of the population had received at least one vaccine; six months later that number rose to 85 percent.
Although Black Democrats were vaccinated at a lower rate than white Democrats, the values associated with vaccine hesitancy follow the lines of partisan values and ideological orientation. A Michigan study in early 2021 found the following:
. . . in the initial wave of the outbreak in May 2020, Blacks experienced more severe direct impacts: they were more likely to be diagnosed or know someone who was diagnosed, and more likely to lose their job compared to Whites. In addition, Blacks differed significantly from Whites in their assessment of COVID-19's threat to public health and the economy, the adequacy of government responses to COVID-19, and the appropriateness of behavioral changes to mitigate COVID-19's spread. Although in many cases these views of COVID-19 were also associated with political ideology, this association was significantly stronger for Whites than Blacks.
The study found that Black Michiganders had more at stake, and more to lose. They were more likely to be infected with COVID-19, so they were also more likely to adopt behaviors of compliance. A history of racist mistreatment, however, affected their compliance. Those who perceived the impact of COVID-19 as less threatening were less willing to comply with mitigating behaviors. The Michigan study demonstrates how that state is a microcosm of the United States. According to data from mid-2021, the top twenty-two states with the highest adult vaccination rates voted for Joe Biden in the 2020 presidential election, and some of the least vaccinated states were the most pro-Trump. This partially explains the influence that Trump had (and arguably still has) on perceptions of vaccine validity and necessity.
But major resistance remained: in September 2021, 35 percent of the eligible US population remained unvaccinated and of that group, 83 percent said they did not plan to get the lifesaving shots. By the end of 2021, 73 percent of adults eighteen and older had received at least one dose of a Covid vaccine, however, 27 percent remained unvaccinated. Of those, 42 percent reported that they "don't trust the vaccine." Vaccine hesitancy, racial inequities in distribution, and state and local disparities in healthcare funding and facilities, continued to impede vaccine delivery as first the Delta variant and then Omicron took their deadly and debilitating toll.6Staff, "A Timeline of COVID-19 Vaccine Developments in 2021," AMJC, June 3, 2021, https://www.ajmc.com/view/a-timeline-of-covid-19-vaccine-developments-in-2021.
In contrast to the Covid geographies of the US, Brazilians appeared to "love vaccines," as Lucas Fontainha wrote in Undark, a digital magazine exploring the intersection of science and society. "They fight for vaccines," he continued, "they throw vaccine festivals, they kiss all the babies in the line waiting for vaccines, they camp overnight at the clinic to get a vaccine . . . even the anti-vaccination Brazilians vaccinate in secret."7Kiratiana Freelon, "Opinion: In Brazil's Successful Vaccine Campaign, a Lesson for the U.S," Undark, October 14, 2021, https://undark.org/2021/10/14/in-brazil-successful-vaccine-campaign-lesson-for-us/.

Unlike Americans in the US, Brazilians have benefitted from robust public health programs and a strong vaccine infrastructure since the 1970s. That said, throughout the pandemic, Brazilians have had to contend with Jair Bolsanaro, the "Trump of the Tropics," a man filled with authoritarian vitriol and disregard for vaccine science. Many worried that his influence would deter vaccine uptake, especially because 55 percent of the country voted for him. Bolsanaro's sphere of influence remains significant. His lukewarm stance on Covid vaccines and his refusal to pre-order them in 2020 and early 2021, resulted in many deaths. Nevertheless, a citizenry that believes healthcare is a basic right has countermanded Bolsonaro's failure of leadership. As the number of Brasilians dying from Covid increased to over 600,000 in 2021, citizens largely ignored their president, eschewed their free choice option to not vaccinate, and lined up for the shots.8Felicia Marie Knaul, Michael Touchton, Héctor Arreola-Ornelas, et al, "Punt Politics as Failure of Health System Stewardship: Evidence from the COVID-19 Pandemic Response in Brazil and Mexico," The Lancet Regional Health: Americas 4 (2020), https://www.thelancet.com/journals/lanam/article/PIIS2667-193X(21)00082-X/fulltext.
In 1973, Brazil created a national immunization program (Programa Nacional de Imunizações) that led to the near-eradication of polio and measles by 2000.9"National Immunization Program–Vaccination," Ministry of Health, accessed July 6, 2022, https://www.gov.br/saude/pt-br/acesso-a-informacao/acoes-e-programas/programa-nacional-de-imunizacoes-vacinacao. This successful program has been strengthened by the creation of a universal healthcare and public health system (Sistema Único de Saúde or SUS) that invested (in-part) in the delivery of free public healthcare, including vaccinations to every Brazilian, codified by the Brazilian Constitution of 1988.10Jairnilson Paim, Claudia Travassos, Celia Almeida, et al, "The Brazilian Health System: History, Advances, and Challenges," Lancet 377, no. 9779 (2011): 1778–97, https://pubmed.ncbi.nlm.nih.gov/21561655/. Vaccine delivery to Brazilian citizens is integrated into everyday life and normalized through informal connections, familiarity, and hyper-locality. Although Bolsanaro rejects the idea that the nation state owes a responsibility to its citizens, the state and local arms of the government (and the Constitution), disagree.11Vincent Bevins, "Despite Bolsonaro, Brazil Has Barely Any Anti-Vaxxers," Intelligencer, November 10, 2021, https://nymag.com/intelligencer/2021/11/despite-bolsonaro-brazil-has-barely-any-covid-anti-vaxxers.html. Not only is the state obligated by law to distribute free services and pharmaceuticals, but citizens are mandated to be part of the process. Even those who choose private insurance must get their vaccines at SUS.














Even when an anti-science president such as Bolsonaro rails against vaccines, there is almost no way for the population to avoid receiving inoculations. In August 2021 in the city of São Paulo, the campaign Virada da Vacina reported that 99 percent of the adults in the city had been vaccinated (Bolsonaro won approximately 45 percent and 60 percent of the vote here in the run offs and general election respectively).12Isabella Menon and Paulo Eduardo Dias, "São Paulo Approaches 99% of Adults with the First Dose of the Covid Vaccine," Folha De S.Paulo, August 15, 2021, https://www1.folha.uol.com.br/equilibrioesaude/2021/08/sao-paulo-se-aproxima-de-99-dos-adultos-com-a-primeira-dose-da-vacina-contra-a-covid.shtml; "See the Calculation Map of all Cities in Brazil," Fohla De S.Paulo, October 7, 2018, https://www1.folha.uol.com.br/poder/eleicoes/2018/veja-o-mapa-de-apuracao-de-todas-as-cidades-do-brasil/?#/cargo/presidente/local/sao-paulo/turno/1/mapa/estadual/municipio/sao-paulo/3550308. Six-hundred locations dispersed the vaccine; sixteen of these were open for walk-in or drive-up around the clock. The state provided DJs, dancing, bands, and artists on stilts to create a carnivalesque atmosphere for those waiting hours in line.
Vaccine culture in Brazil is about accessibility. Locals become part of the campaign. That means you are likely to know and have some regard for the person who comes to you in the name of immunization—in the metro stations, on street corners, or in the park. Public displays boost the vaccine's image. It is harder to retreat into spaces of disinformation when the people you know, or even don't know, seem open to receiving a vaccination. A 2021 study showed that even among vaccine-hesitant individuals in Brazil (10.5 percent of the sample), only 2.5 percent did not intend to vaccinate at all.13Daniella Campelo Batalha Cox Moore, Marcio Fernandes Nehab, Karla Gonçalves Camacho, et al. "Low COVID-19 Vaccine Hesitancy in Brazil," Vaccine 39, no. 42 (2021): 6262–6268. Still, a June 2022 report from The Lancet found that municipalities that supported Bolsonaro in the 2018 elections were those that had the worst COVID-19 mortality rates, especially during the second epidemic wave of 2021.

As of June 2022, 87.3 percent of Brazilians have received at least one dose of COVID-19 vaccine and 79 percent have been fully vaccinated, compared with 79.8 percent of US citizens having received one dose and 67.5 percent being fully vaccinated.14COVID-19 Vaccination Tracker, Reuters, last updated July 15, 2022, https://graphics.reuters.com/world-coronavirus-tracker-and-maps/vaccination-rollout-and-access/. While these numbers are not vastly different, it is of note that Brazil President Bolsonaro remains in power, regularly flouting vaccine regulations and bragging about his unvaccinated status, whereas since 2021 in the United States, President Joe Biden has worked tirelessly to get vaccines in arms, bolster public health, and eliminate health disparities.15Rodrigo Pedroso, "Brazil's Bolosnaro Says He Will Not be Vaccinated Against Covid-19," CNN, October 13, 2021, https://www.cnn.com/2021/10/13/americas/bolsonaro-no-vaccine-intl/index.html; Chuck Todd, Mark Murray and Carrie Dann, "Biden is True to a Key Promise: Getting More Shots in Arms," NBC News, March 19, 2021, https://www.nbcnews.com/politics/meet-the-press/biden-true-key-promise-getting-more-shots-arms-n1261531; HHS Press Office, "Biden-Harris Administration Provides $121 Million in American Rescue Plan Funds to Support Local Community-Based Efforts to Increase COVID-19 Vaccinations in Underserved Communities," HHS, July 27, 2021, https://www.hhs.gov/about/news/2021/07/27/biden-harris-admin-provides-121-million-in-arp-funding-to-local-communities-for-covid-19-vaccines.html.
Early in his tenure, Biden proposed a $1.6 billion increase for the Centers for Disease Control and Prevention to improve core public health capacities in states and territories, modernize public health data systems, train new epidemiologists and other public health workers, and build global capacity to respond to future health threats. Some of these efforts have worked. By August 2021, Pew research reported that around three-quarters of US adults (73 percent) had received at least one dose of a COVID-19 vaccine.
Despite these efforts, too many Americans see vaccine mandates, not as a way toward building public safety, but as extreme government overreach. Republicans and Libertarians have called repeatedly and loudly for "personal freedom" to be prioritized over public safety. Before the Supreme Court blocked the Biden administration's vaccine-or-test requirement for large private businesses in January 2022, there was an outcry for #massnoncompliance. Some scholars have called this political resistance to vaccines based on the tenets of choice and liberty, a "uniquely American predicament."16Alana Wise, "The Political Fight Over Vaccine Mandates Deepens, Despite their Effectiveness," NPR, October 17, 2021, https://www.npr.org/2021/10/17/1046598351/the-political-fight-over-vaccine-mandates-deepens-despite-their-effectiveness. And while the oppositional forces of conservatism and science have been noted as phenomenon elsewhere, including Brazil, the lack of a dominant US culture that trusts and respects public health and expects that the state can and should deliver it can be attributed largely to decades of right wing ideologues across many forms of media.
To date, an Omicron subvariant (BA-5) is the newest variant of concern, threatening a wave of infections and reinfections. As we continue to navigate this global pandemic, we must pay attention to the true influencers of public health. In Brazil, the public health system has a strong history of emboldening citizenry with a message of governmental duty and obligation. We'll see how this may play out in the polls come October for upcoming elections in this country. In the United States, anti-vax politicians, many of whom have themselves received the vaccine for COVID-19, have spread misinformation and anti-government rhetoric about public health. Although conservatism and evangelical religiosity has led to vaccine hesitancy, a Pew Report shows us that most Americans who go to religious services say they would trust their clergy's advice on COVID-19 vaccines. Some advocates of public health have historically prioritized local partnerships with religious leaders and institutions acknowledging this very important sphere of influence.
We must continue to undertake hard conversations about the tensions between individual freedoms and population health much as we did when H1N1 struck our collective shores. As families like my own navigate the implications of a mutating virus that generated a global pandemic, we need trusted resources that are sensitive to historical experiences and the collective common good.
About the Author
Dr. Melissa S. Creary is assistant professor in the Department of Health Management and Policy, School of Public Health at the University of Michigan and the senior director for the Office of Public Health Initiatives at the American Thrombosis and Hemostasis Network (ATHN). She assists ATHN in finding ways to leverage public health research and policy to make a broader impact within the bleeding and blood disorders population. Dr. Creary's areas of specialization include race and racism, genetics, identity politics, health policy, and health equity. She worked for a decade as a health scientist at the Centers for Disease Control and Prevention in the Division of Blood Disorders, has done extensive field work in Brazil, and has more than twenty years of bench, public health, and social science research experience.
Public Health in the US and Global South is a collection of interdisciplinary, multimedia publications examining the relationship between public health and specific geographies—both real and imagined—in and across the US and Global South. These essays raise questions about the origin, replication, and entrenchment of health disparities; the ways that race and gender shape and are shaped by health policy; and the inseparable connection between health justice and health advocacy.
Beginning in 2022, the series expands to include 1000-word blog posts, as well as longer commentaries, essays, articles and media productions that address the public health and political implications of the COVID-19 pandemic from multiple viewpoints. The series editor for Public Health in the US and Global South is Mary E. Frederickson.
Commentary
An online search using the keywords "COVID-19" and "lessons" turns up an astonishing volume and assortment of information: thousands of commentaries, news stories, scholarly articles, book chapters, and monographs. The lessons are intended for vast expert and general audiences: from pediatricians, public health professionals, and other specialized communities of practice to ordinary people and political leaders across the planet. What has been, can be, and should be learned? More lessons loom. Expect a deep dive Congressional investigation and blue-ribbon probes. Storytellers are weighing in with fictional chronicles. Booker Prize winner Ian McEwan's novel, Lessons (New York: Alfred A. Knopf, 2022), is scheduled for September 2022.

From my perspective as a recently retired Centers for Disease Control and Prevention (CDC) branch chief who served in the agency's COVID-19 response from late March through June 2020, the profusion of "lessons learned" reflects the magnitude of the knowledge gaps that impaired America's readiness and undercut its efforts to grapple with a new pathogenic peril, one for which danger signs were long evident. Failures in foresight were followed by fitful attempts at comprehending a lethal contagion's spread and knowing what to do about it.1Cormac Bryce, Patrick Ring, Simon Ashby, and Jamie K. Wardman, "Resilience in the Face of Uncertainty: Early Lessons From the COVID-19 Pandemic," Journal of Risk Research 23, no. 7–8 (2020): 880–887.
The story of the nation's COVID-19 plight is as much an unfolding epistemological crisis as it is a once-in-a-century epidemiological catastrophe. Among the many lessons to be distilled are how and why ignorance in various forms and places accounts for so much of what went wrong. A thorough and wide-ranging exploration is needed, which calls for contributions from multiple disciplines and approaches. As historian of science Robert Proctor recommends: "We need to think about the conscious, unconscious, and structural production of ignorance, its diverse causes and conformations, whether brought about by neglect, forgetfulness, myopia, extinction, secrecy, or suppression."2Robert N. Proctor, "Agnotology: A Missing Term to Describe the Cultural Production of Ignorance (and Its Study)," in Agnotology: The Making and Unmaking of Ignorance, ed. Robert N. Proctor and Londa Schiebinger (Stanford, CA: Stanford University Press, 2008), 1–33. Further, as sociologist Scott Frickel suggests, we also need to focus on "how, where, and why ignorance, once produced, becomes institutionalized."3Scott Frickel, "Not Here and Everywhere: The Non-production of Scientific Knowledge," in Routledge Handbook of Science, Technology, and Society, ed. Daniel Lee Kleinman and Kelly Moore (New York: Routledge, 2014), 263–276. For example, studies of CDC's shambolic performance should include close scrutiny of institutional obliviousness, under a succession of agency directors and programmatic leaders, to basic gaps in readiness and responsiveness that became glaringly obvious during the pandemic and contributed to numerous missteps in the US response to COVID-19.
If the so-called Spanish influenza of 1918 was, in the words of historian Alfred W. Crosby, America's Forgotten Pandemic, then for the time being the bounty of lessons suggests that COVID-19 is America's Teachable Moment Pandemic.4Alfred W. Crosby, America's Forgotten Pandemic: The Influenza of 1918, Second Edition (New York: Cambridge University Press, 2003), 311–328. The largest public health cataclysm in a hundred years has put to the test assumptions, capacities, decisions, practices, and policies. In many ways, the United States has been found wanting, as evidenced by the exceptionally devastating and inequitable toll that COVID-19 has exacted, much of which was averted or more proficiently mitigated by other countries, including nations in the Global South. Vietnam is a prime example.

Events turned US exceptionalism on its head; the nation's heralded public health preeminence ran aground against a novel corona virus. Remarkably, four months before the World Health Organization declared the worldwide spread of COVID-19 a public health emergency, preparedness experts convened by the Nuclear Threat Initiative and Johns Hopkins University reported that the United States was at the top of the heap internationally in terms of its readiness to contend with a pandemic. Scoring 83.5 out of 100 possible points, the US was deemed "best prepared" in the world.5Elizabeth E. Cameron, Jennifer B. Nuzzo, Jessica A. Bell, et al, Building Collective Action and Accountability, GHS Index, October 2019, https://www.ghsindex.org/wp-content/uploads/2019/10/2019-Global-Health-Security-Index.pdf. Yet, when the virus began to spread throughout the nation, political and public health leaders overlooked or failed to respond promptly and effectively to signals of a mounting threat.
Myriad displays of ignorance in preparedness and response cast a spotlight on areas of knowledge, most visible in America's contributions to pathogen genomics and vaccine development, that were the rarity rather than the rule. As historian Peter Burke predicts, much will be said about ignorance when we look back on the pandemic.6Ana R. Rego and Marialva Barbosa, "Interview With Peter Burke: About Ignorance Nowadays," Revista Famecos—Midia, Cultura e Tecnologia 28 (2021): 1–7. The United States will provide many examples for review. "The coronavirus is very much under control in our country," President Donald Trump claimed without justification in February 2020.7"Trump Says Coronavirus Is 'Very Well Under Control' in U.S.," Bloomberg, February 25, 2020, Video, 1:26, https://www.bloomberg.com/news/videos/2020-02-25/trump-says-coronavirus-is-very-well-under-control-in-u-s-video. When cases and deaths surged, corporate America chimed in with commercials proclaiming "we are all in this together," a slogan that blithely disregarded systemic, inequitable differences in exposures, resources, and outcomes.8"Every Covid-19 Commercial is Exactly the Same," Microsoft Sam, April 15, 2020, YouTube video, 3:40, https://www.youtube.com/watch?v=vM3J9jDoaTA. As COVID-19 variants emerged and disease waves swelled, public health officials justified shifts in their response guidance with the catchphrase "follow the science," in effect denying knowledge gaps and glossing over judgment calls that informed their decisions.9Nason Maani and Sandro Galea, "What Science Can and Cannot Do in a Time of Pandemic," Scientific American, February 2, 2021, https://www.scientificamerican.com/article/what-science-can-and-cannot-do-in-a-time-of-pandemic/. Sports celebrities and other influencers joined in; some publicly declined vaccinations for spurious or unspoken reasons. In one widely publicized instance, a National Football League Most Valuable Player invoked vaccine misinformation to justify his decision to remain unvaccinated.10Ken Belson and Emily Anthes, "Scientists Fight a New Source of Vaccine Misinformation: Aaron Rodgers," New York Times, November 14, 2021, https://www.nytimes.com/2021/11/08/sports/football/aaron-rodgers-vaccine.html. These displays of ignorance, from the individual to the federal levels, almost certainly will be among the major topics covered when histories of America's recent past are written and discussed.
To a large extent, first drafts of our national COVID-19 history have been assembled, produced in near real-time amid an evolving pandemic. Among the lengthier accounts are books by Nicholas Christakis, Scott Gottlieb, Michael Lewis, Andy Slavitt, and Lawrence Wright.11Nicholas A. Christakis, Apollo’s Arrow: The Profound and Enduring Impact of Coronavirus on the Way We Live (New York: Little, Brown Spark 2020); Scott Gottlieb, Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next Pandemic (New York: HarperCollins, 2021); Michael Lewis, The Premonition: A Pandemic Story (New York: W.W. Norton, 2021); Andy Slavitt, Preventable: The Inside Story of How Leadership Failures, Politics, and Selfishness Doomed the U.S. Coronavirus Response (New York: St. Martin’s Press, 2021); Lawrence Wright, The Plague Year: America in the Time of Covid (New York: Alfred A. Knopf, 2021). Their narratives and additional reports, published across a wide variety of media platforms and outlets, recount a now familiar cascade of main events: warning signals missed or ignored. Contagion risks initially misunderstood or minimized. Testing bungled. Weaknesses in public health infrastructure and operations laid bare. Guidance delayed, shifted, and politicized. Mandates and masks applied, albeit unevenly. Healthcare stretched to the breaking point. Inequalities exposed. Supply chains disrupted. The economy slackened. Government spending skyrocketed, then dipped. Red-Blue divides widened. Vaccines produced in record time received mixed receptions. COVID-19’s impact surged, subsided, and swelled again—repeatedly. The pandemic dragged on and left its mark virtually everywhere and on everyone.
A bevy of initial accounts present a broad historical outline of what happened—to date. However, potential pitfalls arise when these first reports go beyond chronicling pandemic events and enter the realm of causal interpretations and lessons learned. There, the authors of quick-to-publication stories should tread particularly carefully, recognize uncertainties, and avoid unjustified or imbalanced explanations. Possible missteps include ignoring explanatory information or information sources and failing to acknowledge, or minimizing, the limits of their evidence. The risks of missing the mark are substantial. Causal interpretations skewed towards the unequivocal and unnuanced provide unreliable takeaway lessons and often obscure deeper etiologic factors. Revisions may be forthcoming, but inaugural versions can exert an outsized influence on what endures as the conventional understanding of what happened and why.

A case in point and cause for concern is Michael Lewis's bestselling The Premonition: A Pandemic Story (New York: W.W. Norton, 2021), a fast-paced narrative—a Hollywood movie version reportedly is on the way—that tells the tale of several outside experts who tried to spur CDC insiders to recognize and respond rapidly in early 2020 to signals of the brewing COVID-19 calamity. CDC's performance leaves little doubt that the agency was ill-prepared for the pandemic and made multiple mistakes in its response, including its botched diagnostic testing roll out, guidance fiascos, and acquiescence to political pressures from the White House. The open questions that Lewis takes on are what accounts for these failures and, more broadly, the poor showing by the United States compared with its lofty, pre-pandemic preparedness ranking. His answers are uncomplicated and unequivocal: the talents and recommendations of experts, represented by a small but heroic crew of scientists and physicians whom he profiles, were ignored, and the underlying cause was a lack of public health leadership, exemplified by the failings of the Trump-appointed CDC Director. According to Lewis, Donald Trump himself bears little responsibility for America's anemic response. "As one of my characters puts it," Lewis reports, "Trump was a comorbidity."12Michael Lewis, The Premonition: A Pandemic Story (New York: W.W. Norton, 2021), xiv.
I read Lewis's book closely, concentrating on his account of CDC's poor performance and the lessons to be learned. Notwithstanding his mystifying minimization of Trump's baleful role, Lewis's The Premonition offers a glimmer of hope for revelatory explanations and guidance. "After a catastrophic season, management always huddles up to figure out what needs to be changed," he suggests in his introduction, invoking a football analogy that promises a line of sight into the gap between reputation and results.13Lewis, xv. However, the front office managers are the target rather than the truth tellers in Lewis's narrative.

To tell his story, Lewis mainly relies on a small coterie of outside experts, most prominently a retired Sandia National Laboratories senior scientist who studied the effects of social distancing on mitigation of pandemic influenza, a former assistant director of the California Department of Public Health who warned state officials about the mounting COVID-19 threat during the pandemic's initial phase, and two physicians who helped write a national pandemic preparedness and response plan during the George W. Bush administration and raised early alarms about COVID-19's potentially devastating impact on the United States. High among their recommendations for thwarting a rapidly spreading contagion were school closures, which Lewis describes as one of the "truths" that his informants had discovered long ago.14Lewis, 211. Yet, considering the downsides of school shutdowns and remote learning, cleaving to that plan and putting it into practice in the COVID-19 pandemic was far from an unequivocal success, an important lesson that eludes Lewis and warrants much further attention.
Lewis doesn't make clear whether he sought or used information from CDC responders about the agency's performance. Notably, he doesn't mention any contact efforts or interviews with insiders about CDC's emergency operations. The enormously harmful effects of Trump and his minions were clear to me and many CDC colleagues, as were major internal weaknesses in the agency's response, which Lewis largely ignores. Some of CDC's shortcomings were due to acute managerial and resourcing problems, often recurring or persistent despite multiple attempts at remediation; others reflected longstanding internal and external assumptions, refuted by the agency's woeful performance, about institutional readiness, proficiency, and sustainability in a pandemic. We need fuller accounts of what went wrong and why, including contributions by CDC insiders, to correctly cull lessons and put them to good use.
More broadly, the flaws in Lewis's assessment serve as a reminder that knowledge claims presented as takeaway lessons do not necessarily undo our ignorance. Some "lessons learned" ignore or minimize more compelling understandings of what went wrong and obscure what we ought to know better. The epistemological crisis that compounded the epidemiological calamity threatens to continue in new forms with the writing of pandemic histories and production of Hollywood dramatizations. Still, COVID-19 has the potential to propel high-value learning and positive changes at the individual, organizational, and societal levels.
Among the nation's earliest and most important pandemic lessons is the immense toll that ignorance can take on human lives. As I write this conclusion, American COVID-19 deaths are fast approaching the one million mark, and untold numbers of people who survived the acute phase of their infections are affected by long-term sequelae. Perhaps we now know better the enormity and implications of what was missing in the national efforts to contend with the pandemic, and we will address collectively what science and technology scholar Manjari Mahajan aptly describes as the "complex political and social determinants that anchor a country's public health response and that are critical in ensuring the sustained well-being of a population."15Manjari Mahajan, "Casualties of preparedness: the Global Health Security Index and COVID-19," International Journal of Law in Context 17, no. 2 (2021): 204–214. COVID-19's impact also has been evident in other, more individual lessons and actions. For many Americans, the pandemic has prompted a personal reckoning and welcome revisions in how they take care of themselves and other people in their lives. However, many COVID-19 lessons and changes are likely to fade, including some that are well worth preserving. America's Forgotten Pandemic of 1918 is a prime example of the finite limits on attention spans and memories. In our time, military conflict and other crises or preoccupations are likely sources of competition for mindfulness, efforts at sense making, and shifts in priorities and routines. "Information is no longer a scarce resource," notes sociologist Sheldon Ungar, "attention and interest are."16Sheldon Ungar, "Ignorance as an Under-Identified Social Problem," British Journal of Sociology 59, no. 2 (2008): 301–326. As a result, America's COVID-19 lessons, including those that are forthcoming, are at risk of diminution or disappearance regardless of their value.
The pandemic is a uniquely teachable moment in our history; we can learn from our ignorance and act accordingly. As political scientist Eric Stern reminds us, despite the formidable obstacles to learning from a crisis, great benefits can accrue from lessons that are deeply reflective, methodologically sound, and highly pragmatic.17Eric Stern, "Bridging the Crisis Learning Gap: From Theory to Practice," in Organizing After Crisis: The Challenge of Learning, ed. Nathalie Schiffino, Laurent Taskin, Céline Donis, and Julien Raone (Brussels: P.I.E. Peter Lang, 2015), 257–272. COVID-19 has made ignorance and its negative consequences more visible in America. Fortuitously, at least for the time being, our lessons in ignorance also provide an impetus for new knowledge and, hopefully, momentum towards a more equitable society, stronger commitments to public health and healthcare, and a much greater responsiveness to planet-wide threats.
About the Author
After completing the CDC's Epidemic Intelligence Service training program in 1986, Daniel Pollock worked as a medical epidemiologist at the agency for 35 years. Dr. Pollock led the CDC unit responsible for national surveillance of healthcare-associated infections from 2004–2021, and he served in CDC's COVID-19 emergency response in the spring of 2020 as the Deputy Incident Manager for data and surveillance.
Public Health in the US and Global South is a collection of interdisciplinary, multimedia publications examining the relationship between public health and specific geographies—both real and imagined—in and across the US and Global South. These essays raise questions about the origin, replication, and entrenchment of health disparities; the ways that race and gender shape and are shaped by health policy; and the inseparable connection between health justice and health advocacy.
Beginning in 2022, the series expands to include 1000-word blog posts, as well as longer commentaries, essays, articles and media productions that address the public health and political implications of the COVID-19 pandemic from multiple viewpoints. The series editor for Public Health in the US and Global South is Mary E. Frederickson.
Preface
Digging Our Own Graves, first published in 1987, concluded with an ominous prediction: "Black lung disease awaits the younger generation of coal miners who are now at work underground." Would that I had been wrong! Today, not only do coal miners still suffer from this lethal but preventable lung disease, they do so at younger ages, some even in their thirties, and they are contracting the most advanced form of black lung at the highest rates ever recorded. More than fifty years after the US Coal Mine Health and Safety Act of 1969 imposed a respirable dust standard on the coal industry, designed to prevent black lung, why do such carnage and suffering persist? This updated version of the original book seeks answers to that question.
My own introduction to black lung began in the winter of 1971–1972, when I came to West Virginia to work for the Black Lung Association. I was barely twenty years old. Extraordinary political transformations were in the making: coal miners, miners' wives, and widows were challenging powerful institutions that had once commanded their acquiescence—the hierarchy of the United Mine Workers, the coal operators' association, county political machines, and the Social Security Administration.1The language of "miners' wives and widows" implies that all miners are male. However, since at the least the 1970s, women have worked in the mines, including underground, albeit in small numbers. I use the language of "wives and widows" because most black lung activists use this language in their organizing and their discussion of black lung compensation (e.g., "widows' claims"). For a young college student from the Midwest, these developments in the mountains of West Virginia beckoned with a romantic excitement. Besides, the mountains were my ancestral homeplace; now I could return to them, not on a summer vacation in the backseat of the family car, but on my own.
Working with the older coal miners and impatient young organizers who made up the Black Lung Association at that time was a formative political experience for me. Coming from a long line of southern subsistence farmers and circuit-riding preachers, I was instilled with a righteous, if vague, sense of populism that made me eager to join the struggles of "working people." But neither my political heritage nor my exposure to campus radicals prepared me for what I found in the coalfields of West Virginia: above all, the stark boundaries and clear perceptions of class antagonism. Virtually every coal miner over the age of sixty-five proudly claimed to have "fought in the battle of Blair Mountain with a machine gun" in 1921 to bring the union into southern West Virginia. They were up against the combined forces of coal company guards, the state police, county sheriffs and their deputies, aerial bombers, and, ultimately, the US Army. I was dumbfounded.
Fortunately, it didn't occur to me to write about any of these experiences until my age and the changing times helped to deepen my understanding of what they might mean. In 1978, more than six years after I had first worked for the Black Lung Association, I began the research for a dissertation on the black lung movement. The political atmosphere was altogether different. A reform movement in the United Mine Workers of America (UMWA) had arisen, succeeded in a special election for leadership of the union, then disintegrated; the black lung movement had seemingly disappeared; and a storm of reaction was sweeping the Appalachian coalfields. The setbacks were frightening, but they made possible a more sober and critical perspective on the earlier period of upheaval.

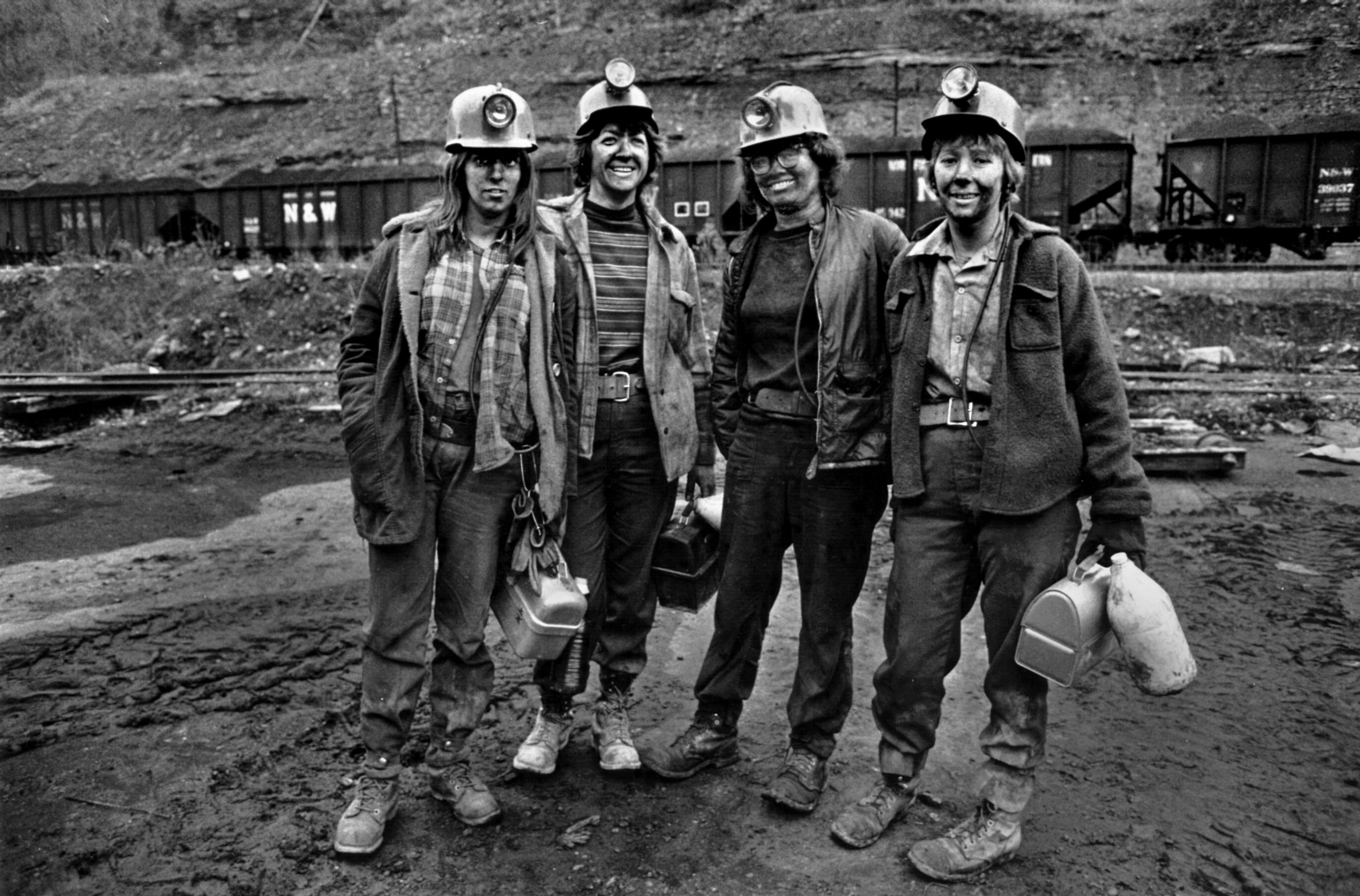

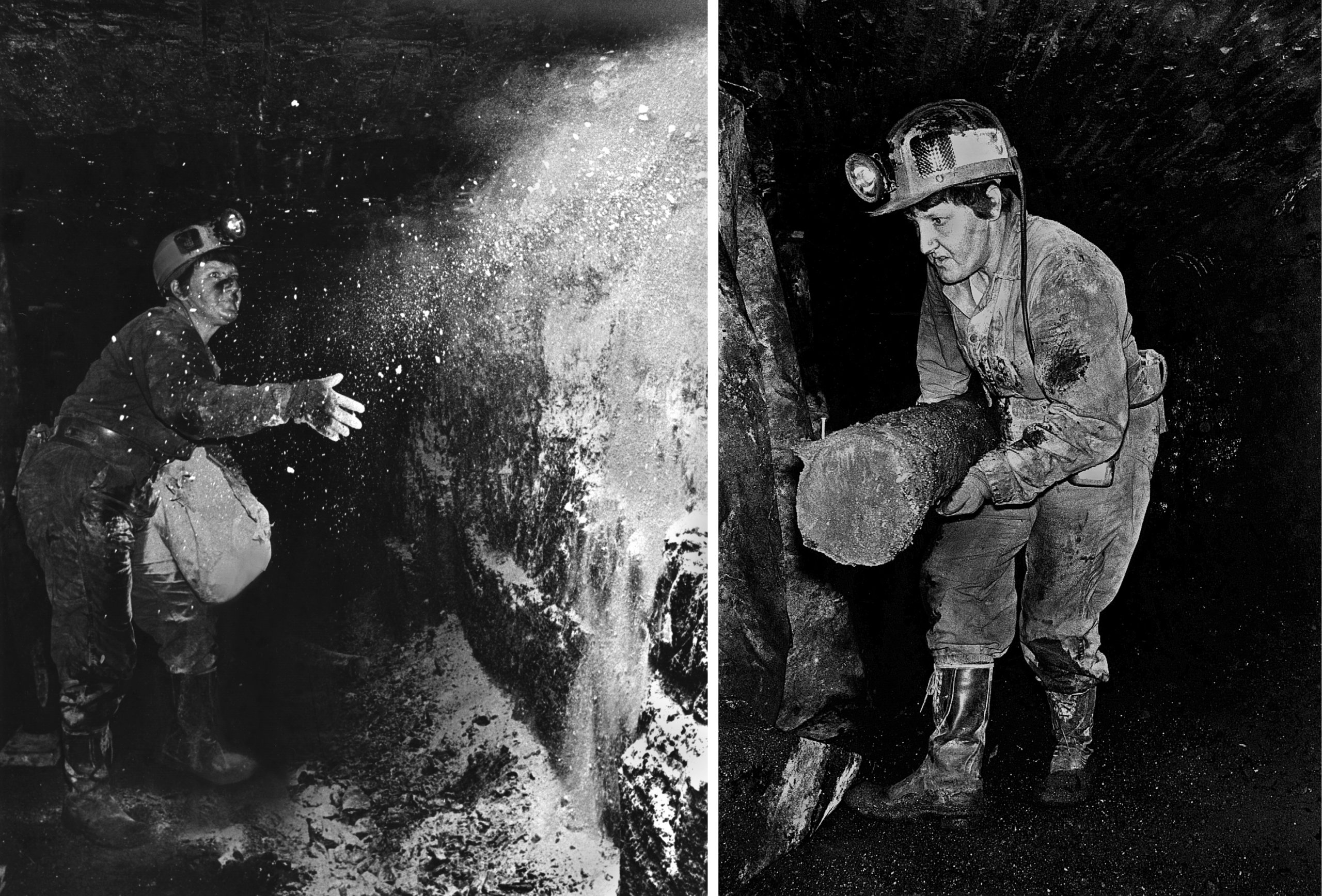
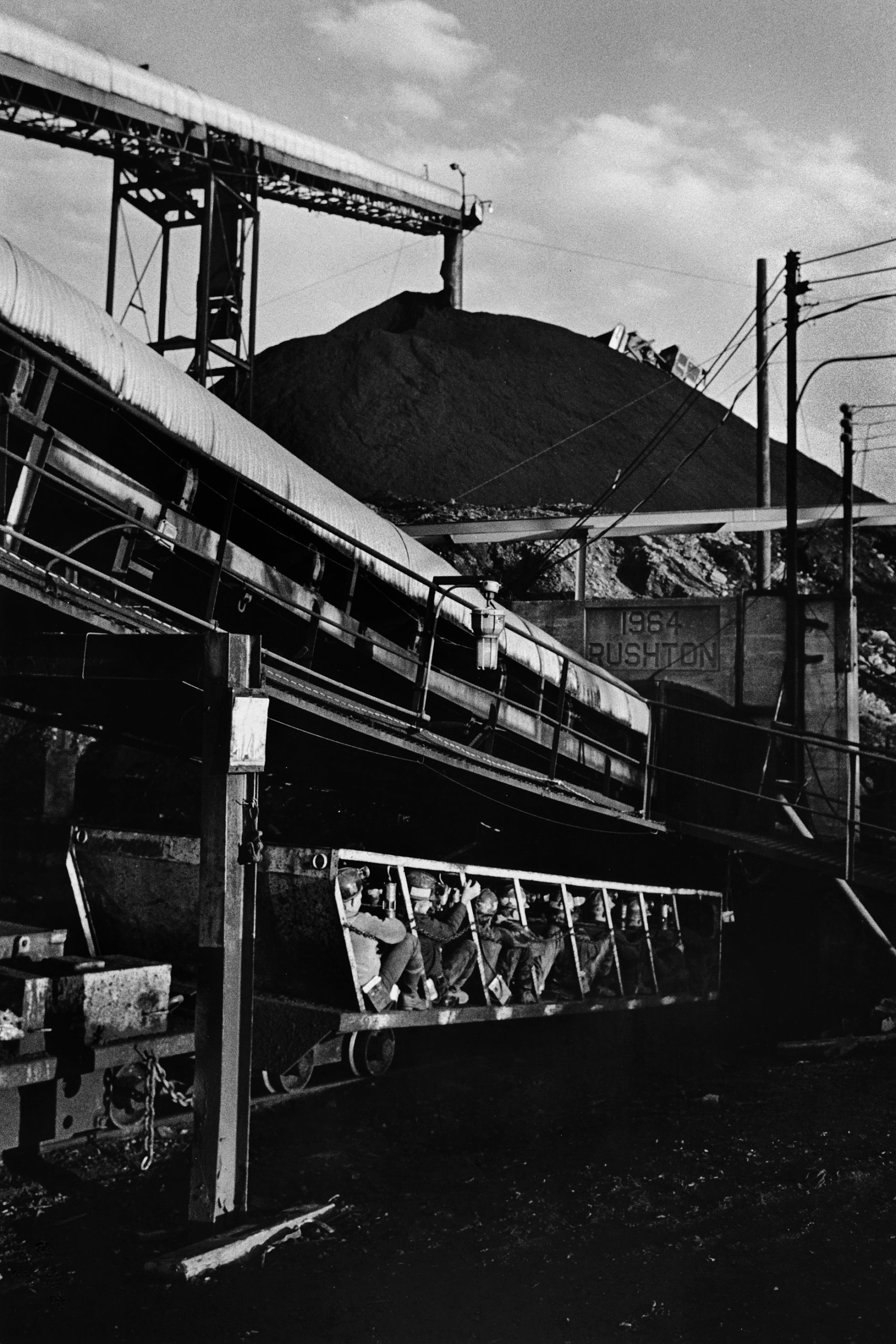





I began this book as a labor history, asking obvious questions that seemed most important at the time: Why did the movement end this way? What did it accomplish? How did it fail? Who or what was to blame? As I dug deeper into the history of the black lung movement, however, these apparently clear-cut questions about victories and defeats began to seem ambiguous, even misleading. The assessment of whether the movement had succeeded or failed depended a great deal on whose goals were used as the standard of measurement—and goals varied considerably among different participants. Moreover, what the larger political culture defined as the movement's greatest accomplishments often turned out to be mainly symbolic; they represented the visible outcomes of formal processes of reform (the passage of legislation, for example), but in and of themselves did not necessarily signify substantial and lasting change. The simplicity of my original questions faded as the labels of victory and defeat, success and failure, appeared more and more ephemeral. The central analytical problems increasingly seemed to involve the maddening complexity of social change itself, which prevented any person or group from controlling the course or outcomes of this movement.
As I delved further into the reforms sought and controversies engendered by the black lung movement, it became apparent that the movement was more than an important episode of labor resistance. At issue in the struggles over black lung, which have reemerged today, is not only how to prevent the disease or compensate those affected by it but also the very definition of black lung. Frequently, the most ideologically powerful opponents that miners have faced in their successive surges of activism are not coal operators or conservative politicians but physicians. At the center of the black lung controversy has been a profound power struggle between miners and physicians over who will control the definition of this disease.2See Daniel M. Fox and Judith F. Stone, "Black Lung: Miners' Militancy and Medical Uncertainty, 1968–1972," Bulletin of the History of Medicine 54, no. 1 (1980): 43–63, for an early framing of the black lung struggle as between miners and physicians over the definition of disease. Their emphasis on medical uncertainty differs from the analysis in my own article, which came out during the same time period: Barbara Ellen Smith, "Black Lung: The Social Production of Disease," International Journal of Health Services 11, no. 3 (1981): 343–359.
As a result of these and other shifts in emphasis, this book is a hybrid. It draws on diverse theoretical traditions in order to analyze not only the organization and development of the black lung movement, but also the history and conflict that underlie the brutal fact of coal miners' diseased bodies. Beginning with how and why black lung originates in the workplace, this book also explores the medical history of the disease and the conflicting meanings that miners and certain physicians, lawyers, and government administrators invest in black lung.
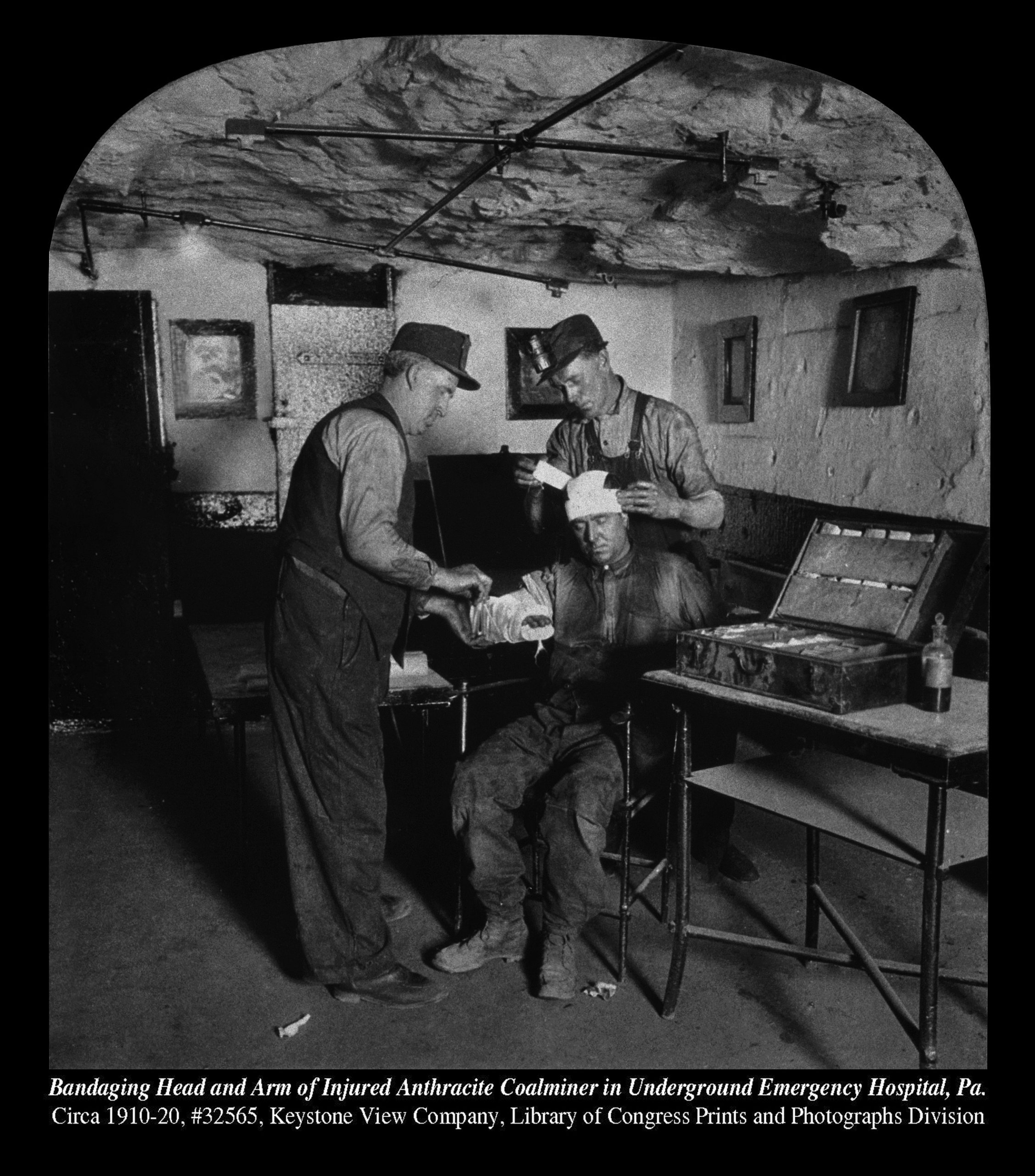
After moving away to a self-imposed exile some twenty-five years ago, I live once again in West Virginia. Contrasts with the 1970s heyday of working-class activism are evident throughout the rural landscape of abandoned gas stations, rusted coal tipples, and boarded-up union halls. The differences are personal as well: when I interviewed black lung activists in the 1970s, I was the age of their daughters and granddaughters; today, I am eligible for Medicare. As I conducted additional interviews in 2019, mostly with retired coal miners close to my age, their bodies as well as their words spoke the story of black lung disease and the physical toll of hard-labor jobs. Conditioned as a white woman to thinking of my embodiment primarily in terms of gender, I was struck again and again by how the privileges of class have shielded me from harm and become subsumed into my body. This updated and revised book, which includes two new chapters and a moving, evocative photo gallery by Earl Dotter, thus entails not only additional research into medical, legal, and economic materials relevant to black lung, but also historical reckonings both political and personal.
Today, as I write this preface, the power relations that miners experience on the job are dangerously asymmetrical, and their outcomes grim. Coal miners in southern West Virginia, once the stronghold of the UMWA in central Appalachia, where those who crossed a picket line invited ostracism if not assault, now work nonunion. Coal companies, facing shrinking domestic markets and in many instances bankruptcy, force workers, coal communities, and American taxpayers to bear the costs of their decline. Black lung can only be fully understood as part of this historical moment, when resistance, remarkably, persists. Digging Our Own Graves analyzes the dreadful resurgence of black lung within the long history of efforts to legitimate this disease and make it visible, prevent black lung in the workplaces where it is produced, and extend dignity and a measure of justice to those for whom prevention comes too late.
Conclusion: Class Power, Scientific Authority, and State Regulation
Nearly two centuries have passed since Dr. James Gregory opened up the lifeless body of John Hogg and hypothesized a connection between the miner's blackened lungs, his respiratory disability in later life, his occupation, and his death. For a time, physicians in Britain and the United States continued to investigate the relationship between occupational exposures and miners' respiratory distress. Toward the end of the nineteenth century, however, during a period of tight corporate control in the Appalachian coalfields and an increasingly restrictive scientific understanding of disease, black lung began to disappear from the medical literature of both countries. In the United States, coal miners eventually precipitated renewed medical attention to black lung by winning a union-controlled health care plan for themselves and their families. Even so, coal workers' pneumoconiosis—much less the broader ensemble of illnesses called black lung—was not accepted as a legitimate, occupationally related disease by the medical profession as a whole.3Journalistic and some scientific accounts equate coal workers' pneumoconiosis (CWP) with black lung. However, an essential component of the black lung movement was miners' and their families' struggle to broaden the definition, beyond CWP, of miners' disabling, occupationally related lung disease. Research by physicians and other scientists familiar with and sympathetic to miners and their health has validated this broader definition. See, for example, Edward L. Petsonk, Cecile Rose, and Robert Cohen, "Coal Mine Dust Lung Disease: New Lessons from an Old Exposure," American Journal of Respiratory and Critical Care Medicine 187, no. 11 (2013): 1178–85. Formal recognition required collective political intervention by coal miners themselves.
Even as social and economic factors have impinged on the medical construction of black lung, so have they shaped the actual production of disease. Black lung originates not simply from the physical presence of dust in coal mines, but from the relative power and respective actions of miners and operators, which influence conditions in the workplace. Miners' eventual success in unionization enhanced their collective power in the workplace, but, depending on UMWA leaders' priorities, unionism at times paradoxically undermined miners' capacity to make that workplace healthy and safe. In the years after World War II, the pact between larger operators and the UMWA produced unimpeded mechanization of the production process, high levels of unemployment, forced migration, and occupational death and disability from black lung. However, that industrial collaboration also produced massive rank-and-file upheaval and a successful effort to reform the union. In the present moment, union weakness and miners' lack of bargaining leverage in the workplace, combined with certain operators' endgame maneuvers to extract coal from thinner seams even while pressing for high levels of labor productivity, once again intensify the extent and severity of the disease.
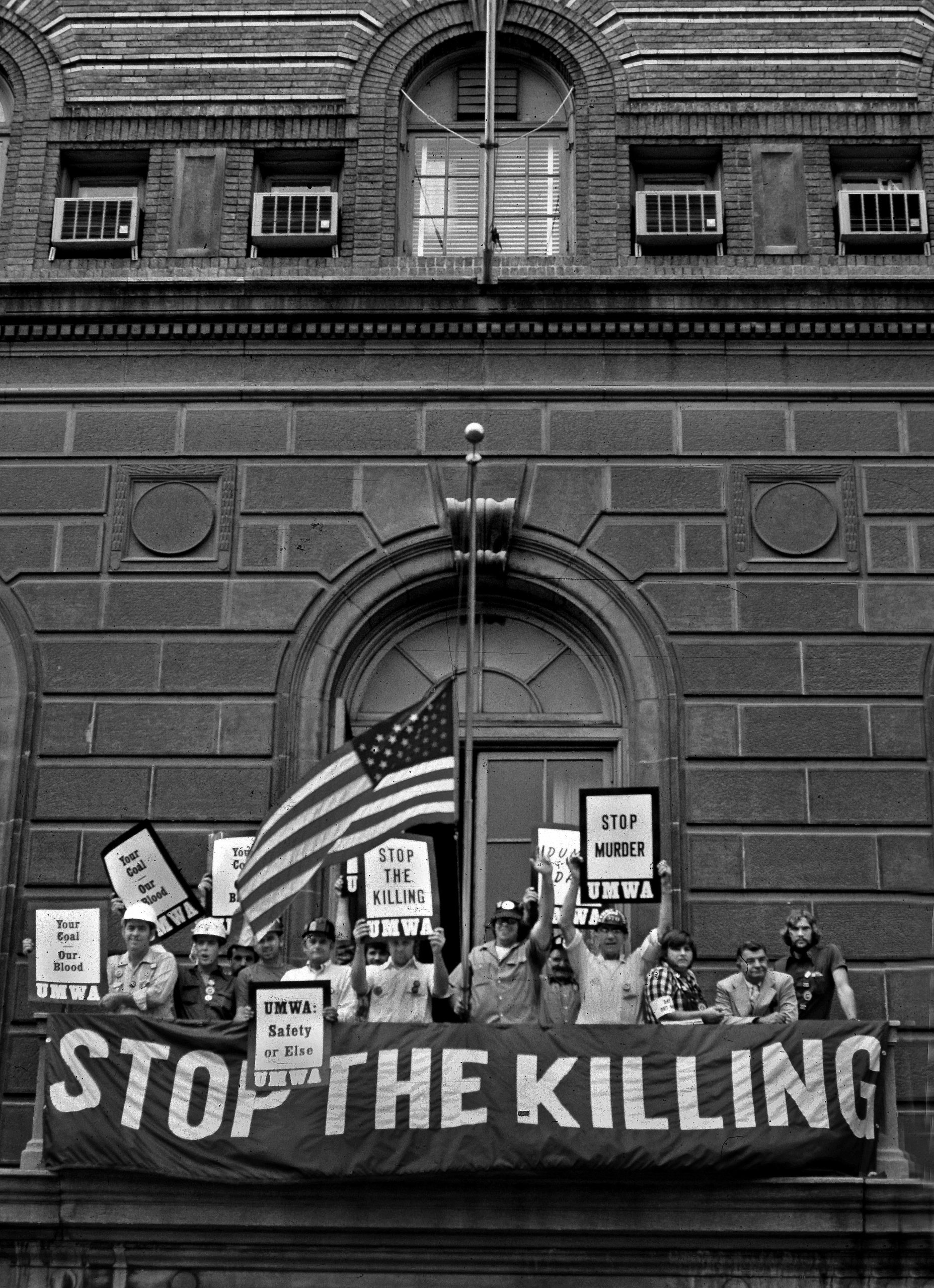





The virulence of black lung today—fifty years after it was supposedly destined for elimination—does not diminish what coal miners, their families, and their allies accomplished in the past. Rather, it attests to the enduring realities of labor exploitation that the black lung movement episodically managed to contest. For its constituents, the movement achieved a unique and unprecedented federal compensation program. Approximately half a million miners and widows have received compensation under the federal black lung program; especially for those ineligible for a pension or other benefits, the monthly payments can mean the difference between destitution and modest survival.4This estimate of the number of black lung beneficiaries is extrapolated from data on the number of claims filed each year, changing approval rates, the annual total cost of claims, and, for some years, reports from the administering federal agency. See, for example, Social Security Administration, Annual Statistical Supplement to the Social Security Bulletin, 2016 (Washington, DC, 2017), Table 9. Beneficiaries who are miners and those who are widows, added together, do not equal the total number of miners judged disabled by black lung, as a widow may receive her husband's benefits after his death. Further, the number of beneficiaries is reported each year as a rolling total, and thus cannot be summed. The coronavirus interrupted my efforts to obtain more precise data. As of December 2018, an individual beneficiary is entitled to receive $660/month, which increases up to a maximum of $1,320 for those with three or more dependents. US Department of Labor, Division of Coal Mine Workers' Compensation, "Benefit Rates Under Part C, 1973–2018," accessed August 16, 2019, https://www.dol.gov/owcp/dcmwc/statistics/PastPartCBenefitRates.htm. The respirable dust standard and other disease prevention measures in the US Coal Mine Health and Safety Act of 1969 are also attributable to the black lung movement. As one element in a larger upheaval throughout the coalfields, the movement contributed as well to the rank-and-file takeover of the United Mine Workers of America and renewal of union leaders' critical attention to occupational safety and health.
Originally and essentially, however, the black lung movement was a struggle over the recognition and, more implicitly, causation of an occupational disease. What seemed at first a straightforward task— achieving legal inclusion of a "new" dust disease under the workers' compensation system—turned out to be a far more complex undertaking. Miners and other activists learned early on that "black lung," as refracted through the lens of scientific medicine, was quite different from the disease for which they sought recognition, compensation, and prevention. In a struggle that has lasted more than fifty years, activists have persistently challenged physicians, lawyers, and policymakers over the meaning of this disease; at different times, they have been able to replace the restrictive scientific construction of a rarely disabling coal workers' pneumoconiosis with their own definition of "black lung." Although focused on arcane disputes over diagnostic methods, disability standards, legal presumptions, and other issues, this conflict over the definition and causation of black lung is intensely political: it involves the ideological content of medicine's view of disease, including the technical perspective that narrows causation to the inhalation of dust, and the powerful role of physicians in labeling work-related disability as legitimate. On the outcome of such conflict rests financial liability for the coal industry that potentially ranges into billions of dollars. The legacy of black lung activism thus entails unsettling questions about the relationship between scientific and technical knowledge, state regulation, and the exercise of class power.
It should be stressed at the outset that not all physicians subscribe to a narrow or purely technical understanding of black lung: recall the role of three doctors (Buff, Rasmussen, and Wells) in the first black lung mobilization during 1968 to 1969 in West Virginia. Dr. Donald Rasmussen continued to work with and advocate for coal miner patients out of his pulmonary lab in Beckley, West Virginia, for five decades, up until his death in 2015.5Sam Roberts, "Dr. Donald L. Rasmussen, Crusader for Miners' Health, Dies at 87," New York Times, August 2, 2015, accessed September 29, 2019, https://www.nytimes.com/2015/08/03/health/research/dr-donald-l-rasmussen-crusader-for-coal-miners-health-dies-at-87.html. Rasmussen's mantle now falls on Dr. Robert Cohen, a pulmonologist who directs the occupational lung disease unit at Northwestern University and frequently testifies before Congress on miners' behalf.6Dr. Cohen testified during the hearings on black lung, "Breathless and Betrayed." See "What is MHSA Doing to Protect Miners from the Resurgence of Black Lung Disease?" YouTube video, 2:58:39, June 20, 2019, House Committee on Education and Labor, https://www.youtube.com/watch?v=sJUDcTf0a_g. Other physicians in the coalfields, such as Drs. Gregory Wagner and Brandon Crum, have devoted much of their professional lives to caring for coal miners with lung disease. After practicing medicine at a clinic on Cabin Creek (West Virginia), Wagner eventually came to direct Respiratory Disease Studies at NIOSH when that agency issued the criteria document that legitimated a broad definition of black lung, inclusive of COPD (chronic obstructive pulmonary disease), and recommended much lower limits on miners' exposure to coal dust and silica.7NIOSH, Criteria for a Recommended Standard: Occupational Exposure to Respirable Coal Mine Dust, publication no. 95–106 (Washington, DC: US Government Printing Office, 1995), xxii, https:// www.cdc.gov/niosh/docs/95-106/default.html. Crum, a radiologist—and, not coincidentally, former coal miner—was first to sound the alarm over black lung's escalating severity, which in 2014 he began detecting among his patients in eastern Kentucky. Four years later, the coal-industry-beholden state legislature responded by disqualifying him from reading X-rays for miners' workers' compensation claims.8Austyn Gaffney, "As Black Lung Strikes Younger Coal Miners, Kentucky Restricts Medical Benefits," NRDC, September 24, 2018, accessed September 29, 2018, https://www.nrdc.org/stories/black-lung-strikes-younger-coal-miners-kentucky-restricts-medical-benefits.
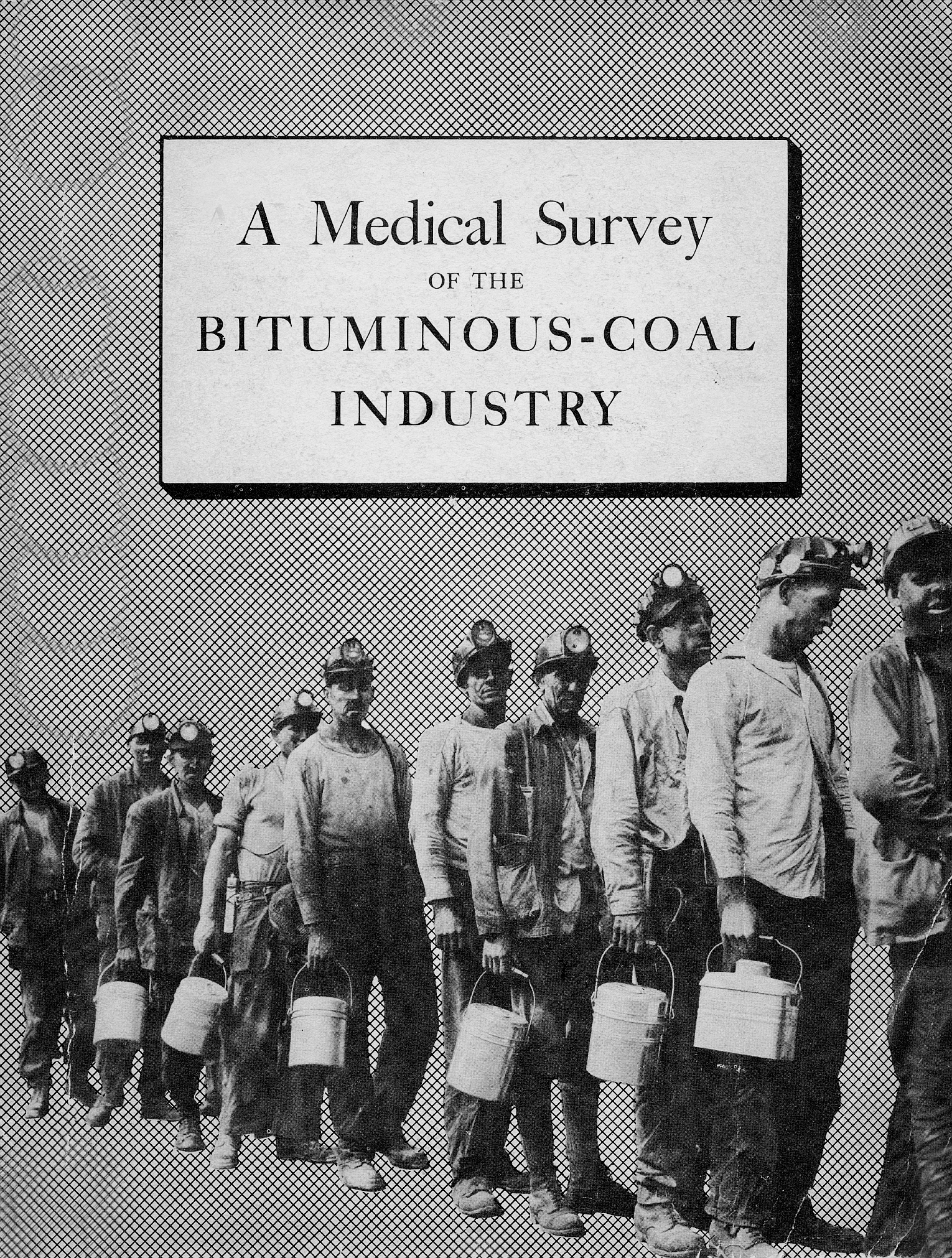




Apart from such individual physicians' political and medical predispositions, however, there remain epistemological tendencies within scientific medicine that militate against the understanding of disease advanced by black lung activists.9This summary of miners' perspectives on the origins of black lung and the role of physicians in advocating a restrictive view of work-related, compensable disease is based on the author's interviews and observations in southern West Virginia at different moments during the past five decades. Within the restrictive medical viewpoint that requires conclusive, scientific proof of occupational causation, black lung is in fact coal workers' pneumoconiosis, a single clinical entity, disabling only in advanced and, even today, relatively rare stages. The disease acquires legitimacy—indeed, effectively comes into existence—only when visible to trained personnel viewing objective diagnostic evidence, that is, X-rays, of an individual miner's lungs. The thousands of miners who believe themselves disabled by black lung yet exhibit no X-ray evidence of advanced CWP might legitimately be considered "disabled"—if the quantitative results of certain tests confirm such a condition. However, the origin of their disability is nonoccupational, above all their own cigarette smoking, or, if nonsmokers, other sources outside the workplace. Although this scientific definition of disease is quite different from physicians' earlier construction of a benign "miners' asthma," the result, in the eyes of many victims, is the same: black lung is trivialized. What many miners view as a collective problem becomes, from the perspective of scientific medicine, individual, quantifiable cases. What they experience as part of the shared social world of coal mining becomes occasional, biological events. What they attribute to their class relationship with the coal operators becomes the product of a single physical agent, dust. In sum, what is collective becomes individual, what is social becomes biological, what is produced by human action becomes the outcome of inert material.
Certain tendencies intrinsic to clinical medical practice are also at stake in the seemingly incommensurable perspectives of miners and certain physicians. Scientific medicine situates disease spatially, within the individual body, and temporally, at the point when signs, symptoms, or other physical alterations develop. Disease is ahistorical as well as asocial; it has no history except a "natural," that is, physical, history. It is said to exist when experienced by the individual and diagnosed by the physician, not at the point when it is being produced. The possibilities for prevention are thus constrained within the very definition of disease.10Howard S. Berliner and J. Warren Salmon, "The Holistic Health Movement and Scientific Medicine: The Naked and the Dead," Socialist Review 9, no. 1 (January–February 1979): 31–52.
Clinical medicine reflects this understanding of disease on a practical level: individual patients present the physician with their distinctive symptoms and complaints; they appear as random, disconnected "cases," and they are granted therapeutic treatment as individuals. There is no social meaning to disease in the sense of an internal relationship between social relations and the individual experience of ill health; primarily individual behaviors, such as diet, exercise, and smoking habits, command attention. Yet, in quantifying disability and allocating it to occupational or nonoccupational sources, physicians implicitly assess the conditions in which miners have lived and worked all their lives. That most physicians have never been in a coal mine (much less worked in one), and that some have never even been in the coalfields, serves to intensify the conflict between physicians and coal miners, who experience the superior legitimacy automatically granted scientific medical knowledge as a complex and powerful form of social control.
The authority of physicians to pronounce miners "healthy" or "disabled" carries important financial consequences. In the context of federal black lung compensation, doctors' assessments of coal miners' health can be decisive in the award or denial of financial benefits that are allocated in large part according to medical eligibility criteria. Doctors act as gatekeepers in a more generic sense as well: they control access to the "sick role," the sole avenue by which adults may legitimately escape the daily responsibilities of their class, race, and gender.11See Talcott Parsons, The Social System (New York: Free Press, 1951). Parsons's conceptualization of the sick role was neither class nor historically specific. For coal miners, as for other workers, the preeminent requirement of their class position is to perform wage labor. Medical criteria for assessing disability (and determining compensation eligibility) that take as the standard for health the functional capacity to work explicitly enforce this requirement. Even if damaged by work, coal miners still must provide medically sanctioned evidence of their "total disability"—i.e., complete inability to continue working—in order to receive financial compensation and legitimate relief from wage labor. In pushing against the limits of this compensation policy, miners and their families implicitly contest not only the ideological authority of physicians to define disease and assess disability; they ultimately threaten the economic power of coal operators by pressing for a broad definition of black lung and relaxed standard of disability that would provide unhealthy miners an alternative to labor in the mines.
This convergence between the restrictive scientific view of black lung and the economic interests of the coal industry is, for many miners and their families, an ultimate source of distrust and conflict with physicians. The narrow definition of disabling black lung as a relatively rare, complicated pneumoconiosis is highly functional to the industry: it circumscribes the scope of occupational lung disease and correspondingly diminishes both the cost of compensation benefits and the importance of prevention. In the context of policy formation, scientific medicine plays a mediating role between the interests of the coal industry and the actions of the state. It facilitates apparent distance between corporate power and public policy, and seems to ground political decision-making in the neutral, technical knowledge of a third party.

The lessons of the protracted struggle over black lung disease encompass both caution and inspiration, loss and hope. In an era of science denialism, when defense of factual truths and scientific knowledge seems obviously necessary, the case of black lung still stands as a warning about the presumed neutrality and appropriate scope of scientific and technical solutions: beware of technical fixes for problems that ultimately derive from economic exploitation and grossly unequal political power. Activists' original quest for redress through the workers' compensation system offers a related caution: the sprawling administrative machinery of the state, which presents the customary, sanctioned route for institutionalizing reform, entails embedded interests that can thwart activists' aims even as it seems to grant their demands. Finally, the long history of black lung suggests that effective prevention of occupational disease, injury, and death ultimately resides in the ever-changing power relations of the workplace and workers' collective, organized capacity to defend themselves. For these and many other reasons, victories are never secure, achieved once and for all; they must be defended, expanded, critiqued, and revised, as black lung activists have doggedly done for some five decades now.
Today, the industry that for more than a century has defined central Appalachia is dying. Those who would chart a post-coal future must grapple with the industry's legacy of incalculable human and environmental destruction, but they would do well to learn from the additional legacy of coal mining families' solidarity and resistance. Ever since the first investors laid claim to the coal of Appalachia, the people of this region have been revolting in various forms against the appropriation of their land, their labor, and even their lives. Those who fought in the black lung movement are both heirs and contributors to this long history of resistance. Today, many miners pay the cost of coal production in the currency of their very breath, but they also continue to resist. Danny Whitt: "We don't never give up. You know when I'll stop? When the last breath leaves my body."12Author's interview with Danny Whitt, Matewan, WV, September 4, 2019.
About the Author
Barbara Ellen Smith is professor emerita of women's and gender studies in the Department of Sociology at Virginia Tech. She has been active in and writing about movements for social and economic justice in Appalachia and the US South for more than 45 years. Her recent publications include a co-edited book with Stephen L. Fisher, Transforming Places: Lessons from Appalachia (University of Illinois, 2012) and Digging Our Own Graves: Coal Miners and the Struggle over Black Lung Disease (Haymarket Books, 2020).
]]>Christina Sharpe, scholar of English literature and Black studies, articulates the concept of "the wake" as a way of thinking about the long term impact of slavery upon African American life. In her work on symbolism in African American literature and visual culture, Sharpe argues that the wake symbolizes the "endurance of anti-Blackness . . . the on-going problem of Black exclusion from social, political and cultural belonging; our abjection from the realm of the human."1Christina Sharpe, In the Wake: On Blackness and Being (Durham, NC: Duke University Press, 2016). More than a metaphor, and sparing no spaces or institutions, the wake exemplifies the ways that white people have constructed African Americans as deviant, criminal, and pathological. As much as any professional group, medical practitioners have contributed to the construction of African Americans as physically, intellectually, and mentally inferior to white people.2Rana A. Hogarth, Medicalizing Blackness: Making Racial Difference in the Atlantic World (Chapel Hill: University of North Carolina Press, 2017); Christopher D. E. Willoughby, "Running Away from Drapetomania: Samuel Cartwright, Medicine and Race in the Antebellum South," Journal of Southern History 84, no. 3 (August 2018): 579–614; Sharla Fett, Working Cures: Healing, Health and Power on Southern Slave Plantations (Chapel Hill: University of North Carolina Press, 2002); Todd Savitt and James Harvey Young, Disease and Distinctiveness in the American South (Knoxville: University of Tennessee Press, 1988); Marli F. Weiner with Mazie Hough, Sex, Sickness, and Slavery: Illness in the Antebellum South (Urbana: University of Illinois Press, 2012). These attitudes continue to plague current approaches to health care, so that many African Americans live every day in the wake of racism that shapes their physical and mental health.
Recently historians have begun to consider the role of psychiatry in the making of these disparities, exploring the intersection of racism and mental health in Harlem, Pennsylvania, and Washington, DC.3Dennis Doyle, Psychiatry and Racial Liberalism in Harlem 1936-1968 (Rochester, NY: University of Rochester Press, 2016); Jay Garcia, Psychology Comes to Harlem: Rethinking the Race Question in Twentieth-Century America (Baltimore, MD: Johns Hopkins University Press, 2012); Martin Summers, Madness in the City of Magnificent Intentions: A History of Race and Mental Illness in the Nation's Capital (New York: Oxford University Press, 2019); Martin Summers, "'Suitable Care of the African When Afflicted with Insanity': Race, Madness and Social Order in Comparative Perspective," Bulletin of the History of Medicine 84, no. 1 (2010): 58–91; Matthew Gambino, "'These Strangers within Our Gates': Race, Psychiatry and Mental Illness among Black Americans at St. Elizabeth's Hospital in Washington DC, 1900-1940," History of Psychiatry 19, no. 4 (2008): 387–400; Gabriel N. Mendes, Under the Strain of Color: Harlem's Lafargue Clinic and the Promise of an Antiracist Psychiatry (Ithaca NY: Cornell University Press, 2015); Anne E. Parsons, From Asylum to Prison: Deinstitutionalization and the Rise of Mass Incarceration after 1945 (Chapel Hill: University of North Carolina Press, 2018). This scholarship builds on the work of psychiatrist and historian Jonathan Metzl. At the Ionia Asylum in Michigan, Metzl documented the ways that the diagnosis of schizophrenia began to skew disproportionately towards Black men in the wake of the Civil Rights movement. Metzl argues that this was an intentional act occurring at the same time as pharmaceutical advertising which cast the Black man as pathologically aggressive, rather than rightfully angry.4Jonathan M. Metzl, The Protest Psychosis: How Schizophrenia Became a Black Disease (Boston, MA: Beacon Press, 2010). Besides Peter McCandless's study of insanity in South Carolina,5Peter McCandless, Moonlight, Magnolia and Madness: Insanity in South Carolina from the Colonial Period to the Progressive Era (Chapel Hill: University of North Carolina Press, 1996). little scholarship has centered on southern states. Two recent books by Wendy Gonaver and Mab Segrest explore some of this missing history. Gonaver's The Peculiar Institution and the Making of Modern Psychiatry 1840–18806Wendy Gonaver, The Peculiar Institution and the Making of Modern Psychiatry 1840–1880 (Chapel Hill: University of North Carolina Press, 2018). traces the linked histories of the Eastern Lunatic Asylum and the Central Lunatic Asylum in Virginia in the context of slavery and emancipation. Segrest's Administrations of Lunacy: Racism and the Haunting of American Psychiatry at the Milledgeville Asylum7Mab Segrest, Administrations of Lunacy: Racism and the Haunting of American Psychiatry at the Milledgeville Asylum (New York, The New Press, 2020). deals with the first hundred years of Georgia's Central State Hospital in Milledgeville from its establishment in 1842.8This review uses the words for the mentally ill that are prevalent in the literature at the time which did not differentiate between the developmentally disabled and mentally ill in the same way we do today. Therefore, words like "Lunatic" and "Idiot" appear in both the names of asylums and in medical literature. They used here only in the ways they are used in the original sources. I consider these books together because they deal explicitly with the impact of racial thinking on psychiatric practices and seek to place state hospitals in the broader context of slavery and its consequences. They also present an intriguing comparison in their access and approach to sources. What we can know about the past is always limited by the silences of the archive, requiring the expertise of historians to read between the lines or seek hidden voices elsewhere.9Britt Peterson, "A Virginia mental institution for Black patients, opened after the Civil War, yields a trove of disturbing records," Washington Post, March 29, 2021, https://www.washingtonpost.com/lifestyle/magazine/black-asylum-files-reveal-racism/2021/03/26/ebfb2eda-6d78-11eb-9ead-673168d5b874_story.html. The challenges of the psychiatric archive are well demonstrated by the work in progress related to the Virginia asylums after the Civil War. Both of these books demonstrate the challenges and the potential of reading in and beyond the archives. Gonaver's The Peculiar Institution and the Making of Modern Psychiatry is an intimate and detailed telling of the multiple lives contained within a forty-year history of Virginia's institutions based on a discrete set of sources. Segrest's Administrations of Lunacy is a history of Georgia writ large, a weaving of scattered and disparate sources from official archives to newspaper reportage that demonstrate the pivotal role that the hospital at Milledgeville played in the state's history. Both authors seek to answer larger questions about the relationship between slavery and psychiatry, and the wake created as they trace the impact of racism on the lives of the mentally ill.
Gonaver's book is based on the kind of access to sources that historians dream of. The records from Eastern Lunatic Asylum in Williamsburg, Virginia (still operating as Eastern State Hospital) remained hidden in a storage closet in the patient library of the hospital. Gonaver undertook training as a volunteer to work in the hospital, where she was then given access to the records which she then organized and assembled into a coherent collection now housed at the Library of Virginia. The collection includes correspondence and drafts of reports but also, significantly, personal diaries and journals from both workers and patients—a rare find in the psychiatric archive. Gonaver supplements these materials with records from official state sources as she seeks to demonstrate the complex network of relationships between the asylum and its local antebellum community, and between its second superintendent, Dr. John M. Galt II, and the field of medicine. Gonaver arranges the book both topically and chronologically and in doing so demonstrates the way that debates about slavery, and about Black-white relations, track with the expansion of the asylum.
Established in 1773 as the first public institution for the mentally ill in the US, Virginia's Eastern Lunatic Asylum was initially a small institution that housed three hundred patients when John M. Galt became the superintendent in 1841. Gonaver starts her history of the asylum at this point because Galt took over at a time of reform in the care of the mentally ill and he sought to bring new ideas to the way he ran the institution. These ideas quickly placed Galt at the margins of American psychiatry, largely because of his attitude towards race. Before the Civil War, Eastern Asylum employed free Black and enslaved people as attendants and staff and admitted both Black and white patients. Gonaver explains Galt's approach to having an interracial clientele, in which "no peculiar strictness is observed" in terms of accommodations for Black and white patients.10Gonaver, The Peculiar Institution, 33. In an 1848 report Galt wrote that African Americans would always be a minority of patients anyway, and that he saw no detriment to their intermingling. This attitude reflected the entwined lives of Blacks and whites at that time, especially in settings of health and healing where there were small numbers of Black patients.11Fett, Working Cures. Gonaver warns us not to read Galt's attitude as any kind of emancipatory rhetoric, but as representing the practical reality of running an institution with limited space and funding.12See Summers, Madness in the City of Magnificent Intentions. In his work on St. Elizabeth's Hospital in Washington DC, for example, Martin Summers explains how segregation based on race rather than diagnostic category finally became untenable when the space would no longer hold.

Gonaver's goal is to show that ideas about race and slavery were central to the formation of American psychiatry. The existence of enslaved people as patients or as workers doesn't in itself tell us a great deal about how that process unfolded. To do that, we need to understand more about how psychiatry itself was evolving in the mid-1800s, and here Gonaver unpacks the contradictions in the therapeutic regimen at Eastern Asylum under Galt. The prevalent treatment practice in the more progressive institutions in Europe and the US at the time was known as moral therapy, which stressed the importance of clean air and physical activity for recovery. Drawing on the example of places such as the York Retreat in the UK, American reformers designed institutions set among acres of landscaped gardens and outdoor grounds.13Nancy Tomes, The Art of Asylum-Keeping: Thomas Story Kirkbride and the Origins of American Psychiatry (Philadelphia: University of Pennsylvania Press, 1984). For paying white patients, moral therapy usually meant walking or light gardening in outdoor spaces, or needlework or carpentry inside. For Black patients, "moral therapy" meant something else entirely, and it is here that we learn the way that mental institutions operated in the wake of slavery. Despite Galt's insistence on 'intermingling,' Gonaver shows that Black patients in Virginia's asylums were effectively separated from white patients through demarcations in labor posing as therapy along lines of race and gender. At Eastern Asylum Black female patients worked in the kitchen and the laundry and Black male patients worked in the fields and farm gardens. This was not work as occupational therapy; it was work as day-long, back-breaking labor without which the institution would not have existed, and the white patients would have gone unfed.
Gonaver describes how Galt used enslaved people to care for Black and white patients, again reflecting patterns of healing relationships that existed on the plantation.14Fett, Working Cures. While Galt did not believe that the African American was equal to the white person in terms of intelligence or emotion, he did defend the work of his Black staff who he felt were just as capable of providing excellent care to patients. This bought him into direct conflict with other psychiatrists, in particular Thomas Kirkbride, a Pennsylvania physician at the vanguard of a movement to reform and modernize the psychiatric institution.15Tomes, The Art of Asylum-Keeping. Kirkbride's large and rambling architectural designs were based on the segregation of patients by gender, race, and diagnostic category. He argued publicly with Galt that it was entirely unsuitable for Black patients to be housed alongside whites, or enslaved people to be used as carers.16Summers, "'Suitable Care of the African When Afflicted with Insanity': Race, Madness and Social Order in Comparative Perspective." Kirkbride's concern was for the reputation of the psychiatric institution. His mission was to sell his new asylum plans to potential buyers (i.e., state governments) concerned with white respectability—the Black patient or attendant was anathema to that idea.
As Galt gave up trying to convince psychiatry's professional bodies of his method's efficacy, Gonaver moves away from an exploration of race relations to include materials that demonstrate intersections with religion and gender. The science of the causes of mental illness in the nineteenth century was hardly precise. Gonaver explores how Galt and his contemporaries were concerned with, as they described it, sensory overstimulation, often taking the forms of excessive religious feeling or female "hysteria." Psychiatry's concern with religious excitement formed part of a large effort to establish scientific knowledge and expertise in place of folk belief (considered superstition), especially in the South in the wake of slavery. This played out in different ways for Black and white patients, and differently again for men and women. As Sharla Fett and other historians have shown, physicians throughout the US were keen to replace traditional healing practices of enslaved Africans as well as the Catholic religiosity of Irish immigrants with what passed for modern scientific rationale.17Fett, Working Cures; Willoughby, "Running Away from Drapetomania;" Deidre Cooper Owens, Medical Bondage: Race, Gender and the Origins of American Gynecology (Athens: University of Georgia Press, 2017). Those deemed excessively religious were barely delineated from the mentally ill in the 1800s and they were frequent admittees to Galt's asylum. His approach to women demonstrated the gender bias inherent to psychiatric and medical practices, where genuine problems such as domestic violence, unhappy marriages, and abandonment were too often read as problems of female hormones. Religious excess in women was considered particularly problematic, as it challenged both domestic and public male authority. Gonaver's discussion of gender speaks to the undercurrent of violence in the nineteenth-century South, the burden of which was borne primarily by Black women. She writes: "The asylum expressly denied women's authority in religious matters, paid inordinate attention to female reproductive organs as the cause of insanity, and promoted a racialized vision of healthy womanhood that ignored the trauma of abuse. In so doing, administrators fostered dependency or passivity in white women, and disproportionately characterized black women as recalcitrant imbeciles, laying the foundation for late nineteenth-century medical and political discourse that . . . portrayed black women as naturally promiscuous."18Gonaver, The Peculiar Institution, 113.


The final chapters of The Peculiar Institution and the Making of Modern Psychiatry deal with the impact of the Civil War on Eastern Lunatic Asylum, which was left vulnerable and chaotic when Galt died from suicide via laudanum overdose in 1862. Caught in the mayhem of Confederate and Union struggles over Richmond and Williamsburg, the asylum was ransacked by both sides. The fate of patients and enslaved workers gave way to broader concerns about the status of freed African Americans in postbellum Virginia. This moment coincided with the emergence of a mental health reform movement across the US. Dr. Kirkbride was assisted in his efforts to reform institutional settings by the work of philanthropic campaigner Dorothea Dix, who advocated for state spending for the construction of new asylums. Neither Kirkbride or Dix cared particularly for the African American patient, and it was in this context that Galt's ideas of an interracial institution came to an end. In 1869, the Freedmen's Bureau took over Howard Grove Hospital in Richmond, and the thirty-six African American patients at Eastern Asylum were moved to this facility. In 1870, it became "Central Lunatic Asylum" and was dedicated solely to the care of African Americans. As Gonaver explains, this was the trend across the country, marking the beginning of Jim Crow segregation in health care. The Peculiar Institution and the Making of Modern Psychiatry concludes with a discussion of how psychiatric discourses about Black patients at the end of the nineteenth century centered around false ideas about biological difference and inherent deviance, setting the scene for a century of neglect, underfunding, and abuse.
This idea that the Black patient was somehow less than human is also a central theme in Mab Segrest's Administrations of Lunacy: Racism and the Haunting of American Psychiatry at the Milledgeville Asylum. Segrest uses Sharpe's metaphor of the "wake of slavery" to explore how a place designed to treat the mentally ill inevitably manifested social relations that were shaped and haunted by the violence of slavery. This is a history that runs in blood and sweat down the walls of Milledgeville—which, as the state of Georgia used the asylum as a dumping ground for a multitude of social problems—housed more than 12,000 people by 1960.
When the Georgia State Asylum for Lunatics, Epileptics and Idiots (sometimes referred to as Milledgeville State Hospital) opened in 1842, racial segregation was central to its design and function. Unlike Galt in Virginia, Milledgeville's first superintendent, David Cooper, knew that racial segregation was essential. As Segrest documents in this vast and ambitious book, administrations of lunacy were also expressions of social relations rooted in dispossession, violence, and white supremacy. Segrest demonstrates the way that people are labelled "crazy" is a function of politics and ideology, in which the meaning of the "South" becomes the cause and symptom of the original disease.
Instead of Gonaver's intensive analysis of the institutional archive, Segrest's work is wider-ranging—due to the kinds of sources she has access to and her own interdisciplinary approach. As a historian, Gonaver strives to stay within the bounds of the archive she has uncovered, and contextualizes that archive with other formal archival sources. While she is theoretically informed and definitely interpretive, the style of writing is much more what we would expect from a "traditional" historian. As a literary scholar, Segrest takes a more creative approach. She builds on work she has written elsewhere about Milledgeville's place in the Georgia imagination—a symbol of the gothic and the grotesque.19Mab Segrest, "The Milledgeville Asylum and the Georgia Surreal," Southern Quarterly; Hattiesburg 48, no. 3 (2011): 114–150,158; Segrest, "Exalted on the Ward: 'Mary Roberts,' the Georgia State Sanitarium, and the Psychiatric 'Speciality' of Race," American Quarterly 66, no. 1 (2014): 69–94, https://doi.org/10.1353/aq.2014.0000. And she is in some ways forced to be so: the records she uses are limited, extending from the mid-1800s to the early twentieth century, and no longer available to the public. They are not systematic or comprehensive institutional records, but contain important fragments from the hospital that Segrest uses to great effect.
Segrest first sets the scene for the antebellum construction of the Georgia asylum, in the small town of Milledgeville that was the state capital at the time. As we saw with Gonaver's history of Eastern Asylum in Virginia, large estates removed from the hustle and bustle of city life were becoming the preferred place for institution-building in the context of moral therapy which stressed the importance of fresh air and clean living for recovery. Milledgeville State Hospital was built in the context of emerging concerns about the poor, indigent, and "feeble minded" as a threat to society. It also emerged at the intersection with new ideas about the capacity of medicine to "cure" the insane, rather than simply hold them in poorhouses.



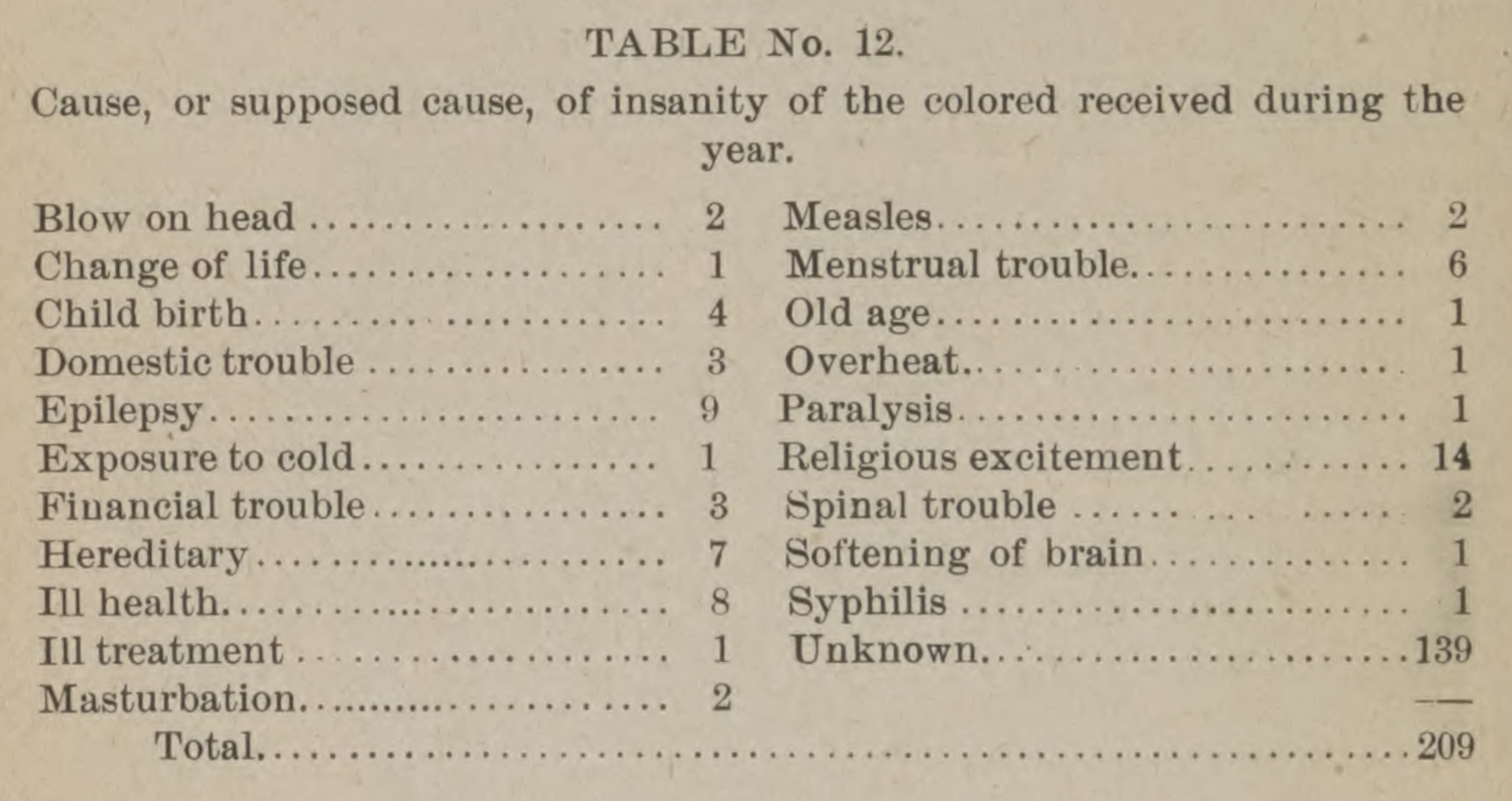


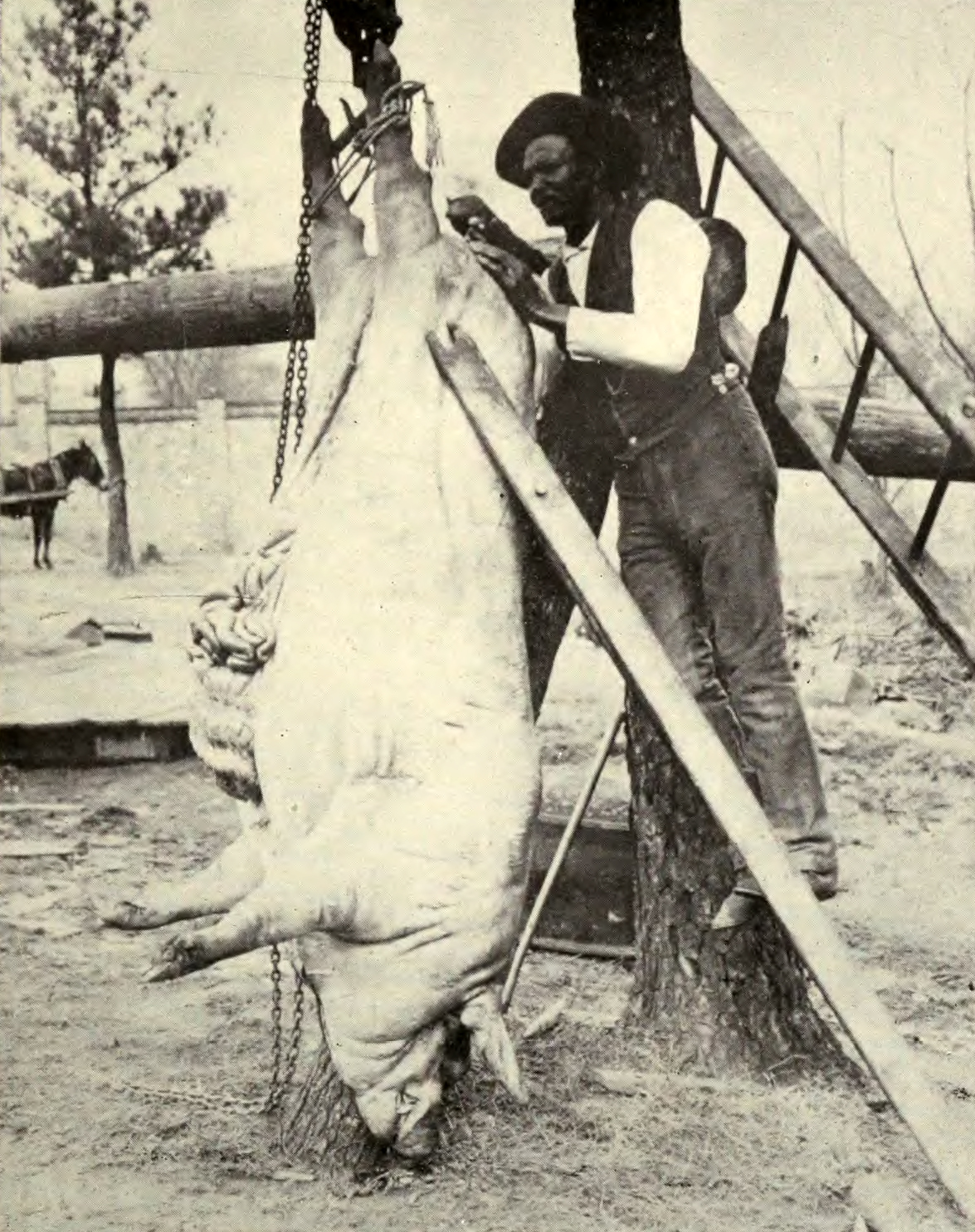









{kind=link}
{kind=link}
Any noble intentions in the establishment of Milledgeville were immediately undercut by the legislature's choice to eschew a Kirkbride-style facility complete with sweeping vistas and sculptured gardens, for the much cheaper single main building which housed all types of patients together, poorly constructed and badly ventilated. And much like Dr. Galt at Eastern Asylum in Virginia, Milledgeville's first superintendent, Dr. Cooper, was his own kind of eccentric. When he sent his first report for publication in the superintendents' association's journal, he made the mistake of telling the truth about his approach to treatment, which was highly aggressive, using all means of restraint at his disposal, and in a style of prose that his northern colleagues found excessive and unprofessional. He earned a severe scolding from the profession's leaders, which saw him removed within his first three years. But, valuable for Segrest, Cooper's report also included extensive case histories. She uses this "opening" to locate the patients he refers to and trace their own histories to tell us something about the lives that brought them to the insane asylum. Her intent is to read "patient narratives through and against the hospital records, newspaper accounts, literary texts, geographical journeys, and oral histories." Her goal is to overlay the history of one hospital with "the dense historical contexts that shaped its patients" and in so doing to write a "restorative history to its Georgia patients, from whose experiences and our own we can continue to understand slavery's afterlives and shape ecologies of sanity in these also turbulent times."20Segrest, Administrations of Lunacy, 10–11.
In order to show connections between the history of the South and the history of psychiatry, and between the past and the present, Segrest divides the book into five parts, from origins of the asylum to "modernity." Each centers around narratives of patients she identified in the records, and whom she traces with diligence through newspapers and census records to place them in their communities and families of origin. This approach serves to humanize the people whose lived experience was shaped by their contact with the Milledgeville Asylum, but it also shows how that asylum itself acted as a tool of social control in the context of white supremacy. The asylum provided substandard conditions for African American patients while it recreated plantation gender roles by putting Black female patients to work in the kitchen and laundry and Black men in the fields. Segrest points out the close relationship between the nearby Georgia Prison Farm. The word "Milledgeville" becomes synonymous with a multitude of ways in which Black bodies can be put to work in what Douglas Blackmon calls "slavery by another name."21Douglas Blackmon, Slavery by Another Name: The Re-Enslavement of Black Americans from the Civil War to World War II (New York: Anchor Books, 2008).
Segrest locates these practices in the context of psychiatric and medical science that itself descended from the plantation. The turn of the nineteenth into the twentieth century bought scientific obsessions with genetics, heritability, and the problem of the feeble-minded for racial purity. Drawing on writings from racist superintendents such as Doctors Green and Powell, Segrest shows how the attitudes about, and approaches towards, Black patients were "new science, old ideas." It is not simply that Black patients were routinely provided with less rations, less clothing, and inferior buildings, but that these conditions were supported by ideologies of eugenics and mental hygiene, justifying the long term confinement and reproductive sterilization of thousands of people whom the elected politicians of Georgia saw as little more than burdens on the state. Segrest demonstrates the impact of new tools such as the Binet IQ Test and the kind of surveys that put the average Georgian IQ at the bottom of national rankings and led to a rise in admissions and sterilizations numbering in the thousands. In this expansion of psychiatric technologies, the asylum acted as a catch-all for Georgia's disabled who were feared and shunned rather than cared for.

Administrations of Lunacy reaches across disciplines and sources making connections between people and institutions where records are often silent. At times Segrest's approach seems a stretch—she can only guess or hypothesize about motivations or connections that are not made explicit in the records. The book is at its best when Segrest stays grounded in the patient case files she is privy to, bringing to life some of Georgia's most forgotten and marginalized people. Because she is not a traditional historian of psychiatry, she glosses over various internal debates within the profession that shaped its mid-twentieth century approach, especially as a consequence of WWII. Her discussion of links to modernity can feel patched together from other sources, moving far beyond the walls of Milledgeville. But again, this is partly due to the limited records available.

Gonaver's primary source collection ends in 1880, Segrest's in the 1920s. While both authors attempt to make connections between their histories and the present situation in psychiatric and mental health care, neither are experts about the incredibly complex array of forces since the 1960s that have created the current set of disparities for minorities with mental illness.22Kylie M. Smith, "How bigotry created a Black mental health crisis," Washington Post, July 29, 2019. https://www.washingtonpost.com/outlook/2019/07/29/how-bigotry-created-black-mental-health-crisis. The community mental health movement of the 1960s led to the closing of massive institutions like the state asylums in Virginia and Georgia. The chronic lack of funding for alternative services has given way to what has been called "trans-institutionalization."23Bernard E. Harcourt, "From the Asylum to the Prison: Rethinking the Incarceration Revolution," Texas Law Review 84 (June 2006): 1751. Attitudes about racial differences continue to plague modern mental health services where Black and minority patients are over-diagnosed with psychotic disorders, underdiagnosed with depressive disorders, and continue to be underrepresented in service utilization data.24M. Alegria, et al., "Disparity in depression treatment among racial and ethnic minority populations in the US", Psychiatric Services, 59 no. 11 (2008): 1264–1272; D. M. Barnes and L.M. Bates, "Do racial patterns in psychological distress shed light on the Black-White depression paradox: A systematic review," Social Psychiatry and Psychiatric Epidemiology, 52 no. 8 (2017): 913–928; J. Breslau, et al., "Racial/ethnic differences in perception of need for mental health treatment in a US national sample," Social Psychiatry and Psychiatric Epidemiology, 52 no. 8 (2017): 929–937. These are national concerns. Many of the problems of Virginia and Georgia's state hospitals were endemic to all large institutions across the US. What Gonaver and Segrest's studies reveal is how the long history and peculiar institutions of Jim Crow segregation ripple through the decades, finding ways to reap themselves on the minds and bodies of Black Americans. Both books are more than partial histories of psychiatry. They are important studies of the ways that institutions such as psychiatric hospitals act as sites through which we can understand broader social relations particular to time and place. They reveal the multiple ways that the wake—the legacy of slavery—continues to shape our national society.
About the Author
Kylie Smith is an associate professor and the Andrew W. Mellon Faculty Fellow for Nursing and the Humanities in the Emory University School of Nursing. She is also associate faculty in the Department of History at Emory University. Her book Jim Crow in the Asylum: Psychiatry and Civil Rights in the American South will be published by the University of North Carolina Press in 2023.
]]>Introduction
. Courtesy of Wikimedia Commons. Image is in public domain.")
In August of 1920, Dr. Oscar Dowling, president of the Louisiana State Board of Health, alerted Governor John M. Parker about the increasing availability of a "powerful narcotic, causing exhilaration, intoxication, [and] delirious hallucinations." Dowling, later chairman of the American Medical Association's board of trustees, also wrote the US Public Health Service urging action to prohibit the spread of this drug throughout the country. Surgeon General Hugh S. Cummings replied to express his "complete agreement" with Dowling's concerns. Governor Parker, surprised to learn there was no federal law curbing the drug, wrote John F. Kremer, prohibition commissioner, and alleged, "two people were killed a few days ago by the smoking of this drug, which seems to make them go crazy wild."1David F. Musto, "The Marihuana Tax Act of 1937," Archives of General Psychiatry 26, no. 2 (February 1972): 102. For more on Dowling, see Richard J. Bonnie and Charles H. Whitebread, The Marijuana Conviction: A History of Marijuana Prohibition in the United States, Drug Policy Classic Reprint from the Lindesmith Center (New York: Lindesmith Center, 1999), 43–44. The drug was marijuana.2Though usually spelled "marijuana" today, "marihuana" was the most common spelling in the United States during the early twentieth century. Different spellings from that period also included: marajuana, mariguana, mariahuana, marahuana, marihuano, mariguana, in addition to other common names like "reefer" and "muggles." For consistency, I use "marijuana" throughout, unless directly quoting from sources with varied spellings.
Dowling and Parker's letters marked the early stages of the "marijuana menace"—a panic that coalesced around the alleged spread of marijuana use among criminals and school-age children in New Orleans between 1920 and 1930. In response, both the city and the state of Louisiana passed laws criminalizing the drug's use, sale, and possession. In the weeks that followed the passage of the city ordinance in 1923, police raided houses, restaurants, and soft drink stands to arrest suspected peddlers and users. Police and the press quickly dubbed users as "muggleheads," drawing on the street term for marijuana. A year later, following unanimous passage by the legislature, Governor Henry L. Fuqua signed a statewide law prohibiting marijuana. In the months and years that followed, civic groups and law enforcement officials in New Orleans launched more than one "muggles drive" and declared "war on dealers in marijuana."3For examples of these enforcement measures, see "Cops Make First Marihuana Raids," Times-Picayune (New Orleans), June 17, 1923; "Marijuana War Is Planned by Mrs. Gregson," Times-Picayune (New Orleans), November 30, 1924, sec. Three; "Ax Killer's Trial Set as 'Muggles' Drive Is Ordered," Times-Picayune (New Orleans), April 18, 1929; "Police Open New War on Dealers in Marihuana," Times-Picayune (New Orleans), October 26, 1930.
Previous studies of marijuana prohibition in the United States have given relatively little attention to city- and state-level events such as these, emphasizing instead developments that led to federal marijuana legislation in 1937.4For prominent examples, see Howard Becker, Outsiders: Studies in the Sociology of Deviance (New York: Free Press, 1963); Alfred Ray Lindesmith, The Addict and the Law (Bloomington: Indiana University Press, 1965); David Solomon, ed., The Marihuana Papers (Indianapolis: Bobbs-Merrill Co., 1966); Donald T. Dickson, "Bureaucracy and Morality: An Organizational Perspective on a Moral Crusade," Social Problems 16, no. 2 (Fall 1968): 143–56; Richard J. Bonnie and Charles H. Whitebread, "The Forbidden Fruit and the Tree of Knowledge: An Inquiry into the Legal History of American Marijuana Prohibition," Virginia Law Review 56, no. 6 (October, 1970): 971–1203; Michael Schaller, "The Federal Prohibition of Marihuana," Journal of Social History 4, no. 1 (October 1970): 61–74; Lester Grinspoon, Marihuana Reconsidered (Cambridge, MA: Harvard University Press, 1971); Musto, "The Marihuana Tax Act of 1937"; David F Musto, The American Disease: Origins of Narcotic Control (New Haven, CT: Yale University Press, 1973). The most influential and widely cited, Richard J. Bonnie and Charles H. Whitebread's The Marihuana Conviction (1974), acknowledges the importance of earlier state laws but offers a limited exploration of their origins or municipal counterparts.5Richard J. Bonnie and Charles H. Whitebread, The Marihuana Conviction: A History of Marihuana Prohibition in the United States (Charlottesville: University Press of Virginia, 1974). For instance, although Bonnie and Whitebread note New Orleans's influential role in fostering marijuana menace ideology, they provide only brief analysis on developments in the city and generally ignore passage of the city ordinance in 1923 and state law in 1924. Rather, they argue that until 1926, "very little . . . was done about the marihuana issue until the press seized upon it."6Bonnie and Whitebread, 44. Likewise, in assessing the city's marijuana users, Bonnie and Whitebread write that "use among black and lower-class white elements of New Orleans emerged along with the propensity toward use by youth."7Bonnie and Whitebread, 92. Moreover, younger users were "drawn from the same socioeconomic classes as the adult users."8Bonnie and Whitebread, 44. They offered little evidence for these claims, and believed New Orleans's officials responded to a general spike in crime during the 1920s by using marijuana as a "convenient scapegoat"—dismissing newspaper and law enforcement claims about the dangers of marijuana and its growing user population in the city as "propaganda."9Bonnie and Whitebread, 67, 71, 92. Bonnie and Whitebread's belief that the city's marijuana users came from fringe and minority groups served to bolster their broader argument that racism and xenophobia played a central role in driving marijuana prohibition nationwide. Despite its limited engagement with evidence drawn from the state and local level, this general interpretation has remained largely unchallenged.10For recent examples that draw heavily from Bonnie and Whitebread's interpretation, see Richard Davenport-Hines, The Pursuit of Oblivion: A Global History of Narcotics, 1st American ed. (New York: Norton, 2002); Martin Booth, Cannabis: A History, First U.S. Edition (New York: St. Martin's Press, 2004); Martin A. Lee, Smoke Signals: A Social History of Marijuana—Medical, Recreational and Scientific (New York: Simon and Schuster, 2013); Johann Hari, Chasing the Scream: The First and Last Days of the War on Drugs (New York: Bloomsbury Publishing USA, 2015). For three notable exceptions that have challenged aspects of Bonnie and Whitebread's conclusions and proved highly influential to my own research, see Jerome L. Himmelstein, The Strange Career of Marihuana: Politics and Ideology of Drug Control in America (Westport, CT.: Greenwood Press, 1983); Dale H. Gieringer, "The Forgotten Origins of Cannabis Prohibition in California," Contemporary Drug Problems 26, no. 2 (Summer 1999): 237–88; Isaac Campos, Home Grown: Marijuana and the Origins of Mexico's War on Drugs (Chapel Hill: University of North Carolina Press, 2012).
In contrast, this essay utilizes contemporary coverage from the Times-Picayune newspaper to analyze the impetus for marijuana prohibition and enforcement in New Orleans as well as the spatial and demographic characteristics of the marijuana users arrested. As one of the earliest urban markets for illicit marijuana use, New Orleans offers an excellent case study for testing prominent aspects of the existing historiography. Given what we now know about marijuana's effects, there is certainly much to critique about the often-hyperbolic commentary on its dangers during the 1920s. Nevertheless, contemporary newspaper coverage sheds light on the origins of those claims as well as the hundreds of marijuana arrests that took place in the city. Many of these reports provided information about the suspects, including their names and arrest locations, the quantity of marijuana seized, home addresses, race, and age. What follows is an examination of the sharp rise in commentary on the dangers of marijuana use alongside an analysis of 225 documented arrests during the first seven years of citywide prohibition. These arrests represent only incidents covered in some detail by the Times-Picayune and provide a valuable database for suggesting patterns and trends among the city's users.11Between May 1923 and December 1929, the Times-Picayune published at least three hundred stories with references to marijuana, roughly one per week. The number of articles mentioning marijuana more than doubled during the subsequent seven-year period. From 1930 through federal marijuana prohibition in 1937, the newspaper published more than six hundred and fifty pieces referencing marijuana, demonstrating the continued growth of public concern with the drug. When combined with an analysis of the simultaneous rise in commentary on marijuana's dangers, this essay and accompanying interactive digital map challenge previous interpretations, revealing both a rapid association between marijuana and crime as well as evidence for a predominately young, white user population that helped drive local concern and provided the impetus for legal prohibitions in New Orleans and beyond.
Youth, Crime, and "Marijuana War"
On February 18, 1922, the New Orleans Times-Picayune announced that a new drug habit was growing rapidly in the city. Citing Dr. Oscar Dowling, who first raised the alarm on marijuana some two years earlier, the newspaper reported the "passage of a drastic law to curb the constantly growing practice of selling and smoking marijuana, also known as muggles, will be sought at the next session of the Legislature." Federal assistance also appeared to be on the way. G. W. Cunningham, chief federal narcotic officer for Louisiana, asserted that, "a measure is to be introduced into Congress which would put marijuana in the same class with morphine, cocaine and opium." Cunningham also "rapped the popular impression that marijuana is not harmful"—suggesting its use may have already reached a critical mass in New Orleans. He believed marijuana "was as habit forming as morphine or cocaine" and that "constant smoking will ruin the health."12"New Drug Habit Rapidly Growing, Health Heads Say," Times-Picayune (New Orleans), February 18, 1922. Though a federal law targeting marijuana use would not pass for another fifteen years, the House Judiciary Committee held hearings on the "Prohibition of Peyote and Marijuana in Interstate Commerce" in 1922.
How much the public knew about marijuana is difficult to assess. In October 1921, a Times-Picayune reader wrote about the paper's recent "allusion to the narcotic preparation of a plant called 'marijuana.'" The reader hoped to learn "where it is grown; its effect on the human system and if it is injurious or otherwise." Such questions suggest a general lack of awareness surrounding marijuana in the early 1920s, but that appeared to be rapidly changing. The newspaper's editorial reply included a range of speculation and confusion alongside information on the effects of cannabis drawn from medical journals. It noted correctly that marijuana "consists chiefly of the flowering tops and tender leaves and stalks of the Indian hemp (Cannabis indica)." Yet, it speculated, "the name 'marijuana' is probably a corruption of the 'majoon' of Calcutta, the name given to the hashish made in that city."13"Questions and Answers," Times-Picayune (New Orleans), October 23, 1921, sec. Two. Furthermore, the editorial connected the word hashish with the etymology of the term "assassin"—an oft-cited legend stretching back to Marco Polo and the Crusades.14For extensive analysis of the link between hashish and Islamic assassins, see Jerry Mandel, "Hashish, Assassins, and the Love of God," Issues in Criminology 2, no. 2 (1966): 149–56; Farhad Daftary, The Assassin Legends: Myths of the Ismaʻilis (London: Tauris, 1994); Campos, "Cannabis and the Psychoactive Riddle," in Home Grown: Marijuana and the Origins of Mexico's War on Drugs, 7–38. Just prior to the passage of the federal Marihuana Tax Act, Harry J. Anslinger, first and long-time commissioner of the Federal Bureau of Narcotics, subsequently made this link famous in "Marijuana: Assassin of Youth," The American Magazine 124, no. 1 (July 1937). The Times-Picayune also included an assessment of the drug summarized from existing medical literature:
The effects differ according to the dose and the idiosyncrasy of the individual. One of the first appreciable effects of the drug is the gradual weakening of the powers of controlling and directing the thoughts. This is followed by dreams accompanied by errors of sense, false convertions [sic], and the predominance of one or more extravagant ideas. A minute may seem a year and an hour only an instant; sounds may be exaggerated, and the sense of duration of time and extent of space and the appreciation of personality are lost. Some individuals become pugnacious, while others fall into a state of reverie. After small doses there is a great tendency to causeless merriment. Although less certain in its action than opium, it is said to possess certain advantages over that drug—that it does not induce torpidity of the liver, create nausea or check the secretions, and it is less likely to occasion headache.15"Questions and Answers."
In short, the Times-Picayune editorial tied marijuana to more familiar forms of cannabis, namely eastern hashish, while ably summarizing some of the existing medical information of the drug.16On the heels of pioneering experiments with cannabis conducted in India by Dr. William Brooke O'Shaughnessy, American physicians began debating the potential merits and dangers of cannabis in the 1840s and regularly published their assessments in prominent medical journals. By the late nineteenth century, most agreed that cannabis could be both helpful and harmful and was therefore in need of legal regulation and medical oversight. Nonetheless, after the turn of the century, ongoing difficulty in standardizing medicinal preparations and occasionally frightening side effects in patients led to steady declines in medicinal cannabis use. For an example promptly assessing O'Shaughnessy's work with cannabis, see W.B. O'Shaughnessy, "New Remedy for Tetanus and Other Convulsive Disorders," The Boston Medical and Surgical Journal XXIII, no. 10 (October 1840): 153–55. On the evolution of American physicians' assessment of cannabis medicines, see Adam Rathge, "Cannabis Cures: American Medicine, Mexican Marijuana, and the Origins of the War on Weed, 1840–1937," (PhD diss., Boston College, 2017), http://hdl.handle.net/2345/bc-ir:107531. It was not a difficult leap to more frightful effects characterized by exhilaration, intoxication, and aggressiveness.
As marijuana moved into the public consciousness of New Orleans in the early 1920s, characterizations of its potentially dangerous effects took hold.17For examples, including comparisons between marijuana addiction and stamp collecting as well as a casual mention of marijuana smoking, see "Just What Is Dishonesty," Times-Picayune (New Orleans), July 1, 1923, sec. One-B; "Literature—and Less—Comments on the Books of the Day," Times-Picayune (New Orleans), July 15, 1923. In May 1922, the Times-Picayune proclaimed "'Muggles' Incites Orleans Youths to Crime" and cited Police Detective Paul R. Maureau who blamed the "Mexican drug" for rash of "outbreaks by boy addicts." Maureau claimed one fourteen-year-old automobile thief was a "member of a gang that was accustomed to smoke 'mirauana' or 'muggles' cigarettes, which are supposed to produce recklessness unrivaled by other 'dope.'" Likewise, a juvenile court judge declared that "several boys have admitted using 'mirauana' to 'get up their nerve' for theft and other offenses." One of the boys testified the drug was available as dried leaves or ready-made cigarettes, purchased for twenty-five cents each. Just one cigarette, claimed Detective Maureau, could "contain criminal inspiration for four or five youths." To solidify the link between marijuana use and crime, Maureau affirmed that a man "arrested recently for the murder of a woman was found to be under the influence of 'mirauana.'"18"Says 'Muggles' Incites Orleans Youths to Crime," Times-Picayune (New Orleans), May 29, 1922.

Stories of marijuana use bolstered fear of its spread, prompting a swift response by the city's commission council. On May 18, 1923, the Times-Picayune highlighted the hospitalization of Randall Sharp—"another victim of the Mexican dope, 'Marijuana.'" Physicians at Charity Hospital "declared there is an epidemic of smoking the contraband in New Orleans and that scarcely a day passes without two or three persons being sent there for treatment." The news story further noted an increase of marijuana "in the city within the last few months."19"Mary Warner Epidemic," Times-Picayune (New Orleans), May 8, 1923. Two days later, at the request of District Attorney Marr and a number of medical professionals, City Commissioner Maloney introduced an ordinance "to make illegal the sale of 'cannabis indica,' better known as 'Mari Juana' or the 'Mexican happy smoke.'"20"Council to Act on Sale in City of Mary Warner," Times-Picayune (New Orleans), May 20, 1923; "Use of Mexican Dope Forbidden by City Council," Times-Picayune (New Orleans), May 30, 1923. On May 29, the council officially prohibited possession and sale of marijuana in New Orleans, with violations punishable by a fine of up to $25 and thirty days of imprisonment.21"Use of Mexican Dope Forbidden by City Council"; "A Yarn of Many Threads," Times-Picayune (New Orleans), July 1, 1923, sec. One-B.
A number of factors contributed to the city's efforts to curb marijuana. The drug was frequently among those sold by street peddlers. Its presence alongside other drugs and alcohol seized during police raids bolstered its prominence.22For two examples, see "Police Capture Weed, Wine and Owners in Raid," Times-Picayune (New Orleans), August 26, 1922; "Drug Ring Hunt Seems to Score," Times-Picayune (New Orleans), December 24, 1922. Early reports on marijuana occasionally noted that it arrived in New Orleans via the city's many shipping docks, often tying the drug to Mexican seamen and foreign vessels.23For example, see "Narcotic Leaves Seized on Vessel," Times-Picayune (New Orleans), September 21, 1922. There was also a quick and clear characterization of marijuana's apparent dangers together with dire warnings about its growing use. Prominent physicians and government officials fostered and reinforced these characterizations, and the purported connections between marijuana use and criminal activity.
Nevertheless, the alleged use of marijuana by schoolchildren appears to have been the primary factor in driving city's prohibitory action. A Times-Picayune exposé entitled "The Victim" chronicled what many believed was happening to an alarming number of youthful users. In the parlor of a former mansion turned tenement, reporter Lyle Saxon sat with the mother of a young boy who wept as she said, "To think that this has happened to my little boy, only twelve years old, and a victim of drugs." Her son Seth and his fourteen-year-old brother had sold newspapers after school. All was well until she "began to notice that something was wrong" with Seth: he "would come home with his eyes wide open, staring, but he seemed half asleep. He would say strange things."24Lyle Saxon, "The Victim," Times-Picayune (New Orleans), June 3, 1923, 20. It is worth noting that while marijuana's effects are often widely varied, its use may have the exact opposite effect on a user's eyes—constricting rather than widening. Known as photophobia, this squint is now a common trope in pop culture references to marijuana use. Many of the tropes in this story appear drawn from the temperance movement. For an exploration of how "eyes wide open" was often used as a symbol of madness linked with marijuana use, see Campos, Home Grown, 155–80. Seth would "sleep like a log" and in the morning, his mother would be unable to wake him up for school. He began missing school entirely and bringing home less and less money from the newspaper sales that helped support the family. When asked, "he couldn't account for where it had gone."25Saxon, "The Victim," 20. Seth also began to "stay out all night," until one day he simply did not come home. Missing for three days, his father went in search of him, eventually "coming home with the boy in his arms, his little head hanging down like he was dead." When Seth's parents called the police, they said he "had been smoking marihuana," or "Muggles."26Saxon, 27.

Social workers, physicians, and local police often confirmed the spread of marijuana smoking among school-age children. The findings of Mrs. Emma B. Stanton, who conducted "an investigation among the small boys and youths of the city," escalated the belief that marijuana was widely available. Stanton claimed that she provided a seven-year-old boy with some money and sent him into a saloon. The boy emerged "a few moments later with a little packet of marihuana, rolled in a bit of newspaper—and with the information that a man inside had offered to roll the cigarettes for him because he was too little to roll them himself."27Saxon, 27. An investigation by Lazu Block, chief attendance officer of parish schools, also found evidence of marijuana use among school-age children. At this news, a collective of more than sixty-three affiliated parent-led education clubs (the President's Cooperative Club) met with the district superintendent and adopted "resolutions approving the efforts of the commission council and the chief of police to stop the sale of marihuana or 'muggles' cigarettes."28"Children Using 'Mary Warner,' Officials Fear," Times-Picayune (New Orleans), June 16, 1923.
In July 1923, the Times-Picayune described "Muggles" as the "boon of newsboys and school children who haven't the means to purchase a more expensive drug."29"A Yarn of Many Threads," Times-Picayune (New Orleans). Reporter Lyle Saxon characterized the situation as especially dire: "to curb the smoking of marihuana is an arduous task—as so many boys and men have acquired the habit, and they will brave almost anything in order to get their daily 'shot.'" Saxon believed "the tragedy of the situation is that this drug is striking at the very roots of society in attacking the children." Marijuana use was quickly "making them slaves, not only to the drug, but to those unscrupulous boys and men who find it to their advantages to 'dope' the children, taking from them their hard-earned pennies, gained by selling papers, shining shoes and so on, leaving the children sleeping in alleys, in gutters and in the streets."30Saxon, "The Victim," 27.
Professional medical opinions urged immediate social intervention and police enforcement, stressing the potential dangers of marijuana. "There is little difference in the effects of marihuana and hashish," said Dr. E. J. DeBergue, assistant city coroner. "When first used it produces a form of mild exhilaration. With constant use this exhilaration passes and one uses the drug simply to feel normal." When compared to "more powerful drugs," DeBergue added, "marihuana gives its addicts an appearance of listlessness, numbness, and a general lack of energy. . . . It produces protracted insomnia and may lead to temporary insanity." In short, marijuana was "intensely harmful."31"A Yarn of Many Threads." Dr. John M. Fletcher, professor of psychology at Tulane University, president of the Southern Society for Philosophy and Psychology, and later chairman of the Louisiana Educational Survey Commission, painted a similar picture of marijuana's dangers. Though not a medical doctor, Fletcher analyzed samples of the drug seized during police raids and summarized the existing, if conflicting, characterizations surrounding it. "In use for centuries as a narcotic stimulant," Fletcher noted the effects were "both mental and physical." Users showed "a gradual weakening of the thought processes, together with extreme errors of sense of time and space." Long-term use led to "indigestion, wasting of the body, cough, melancholy, impotence and dropsy." Eventually, Fletcher claimed, "its votary becomes an outcast from society, and his career terminates in crime, insanity and idiocy."32Saxon, "The Victim," 27.

These grave assessments and the growing fear of marijuana's spread among children fueled calls for additional legislative action. In May 1924, newly elected representative Fred W. Oser, a former police reporter for the Times-Picayune and secretary to the commissioner of public safety in New Orleans, brought the city's desire for marijuana enforcement to the state legislature in Baton Rouge. Oser said he often "observed the evils of marijuana," and one of his first actions was to introduce statewide anti-marijuana legislation.33For Oser's quotes see "Red Sticks—Against Marijuana," Times-Picayune (New Orleans), May 14, 1925, 3; "Bills Introduced," Times-Picayune (New Orleans), May 15, 1924, 2. His proposal, which sought to forbid the sale and transportation of marijuana, carried mandatory provisions for a fine and imprisonment and prohibited the trial judge from suspending the sentence. In early June, the judiciary committee of the House favorably reported on the bill.34"Bill Outlaws Marijuana," Times-Picayune (New Orleans), June 4, 1924, 2. Little more than a week later, Oser presented the bill for a vote and insisted there should be no objection from his colleagues. His fellow representatives declared the bill was "splendid and badly needed," insisting, "such a law is absolutely necessary." Oser's bill swept through the chamber, "84 yeas to no nays."35"House Warms Up to Legislative Work," Times-Picayune (New Orleans), June 13, 1924, 4. On July 1, 1924, Governor Henry L. Fuqua signed the legislation into law. The measure allowed for limited sale of specific medically prescribed cannabis preparations, but otherwise prohibited possession, sale, and transportation.36The law restricted prescriptions to medicinal preparations containing a limited percentage of cannabis extract. "Marajuana Outlawed," Times-Picayune (New Orleans), July 2, 1924, 15; "Bills Signed by Governor Fuqua," Times-Picayune (New Orleans), July 13, 1924, sec. One-B, 5; "Orleans Parish Lawmakers to Tell About It at Dinner," Times-Picayune (New Orleans), July 28, 1924, 3.
Backed by the city ordinance and state law, New Orleans law enforcement agents and civic clubs continued their efforts to curb marijuana use, especially among youth. In May 1925, New Orleans coroner, George F. Roeling urged "police cooperation with his department in endeavoring to trace the source from which persons under his care for observation obtain alcohol, habit-forming drugs and 'muggles.'"37"Mentality Tests for Speeders Urged by Coroner Roeling," Times-Picayune (New Orleans), May 31, 1925, 1. A meeting of the New Orleans Federation of Clubs in November included continued allegations of marijuana use by young children. "Marijuana is being sold in drug stores and candy stores throughout the city," declared Mrs. Emma Bell Stanton. "School boys are smoking this pernicious drug in cigarettes, and school girls, automobile riding at night, are becoming intoxicated by it."38"Women to Fight Marijuana Sale," Times-Picayune (New Orleans), November 25, 1924, sec. Part Two, 17. Mrs. Charles Gregson, chair of the Federation of Clubs committee on anti-narcotics, declared "Marijuana War." The first battle aimed to stop use of the marijuana cigarette—what Gregson called "a stepping stone" toward the "use of even more vicious and degrading narcotics."39"Marijuana War Is Planned by Mrs. Gregson." Gregson's use of the term "stepping stone" here may signal the origins of the "gateway drug" theory that ultimately proved highly influential in bolstering a prohibitory stance on marijuana throughout the second half of the twentieth century. Police Detective Henry Asset stressed that the effects of marijuana were "not so deadly in themselves, but in many instances they lead to the use of more powerful drugs."40"A Yarn of Many Threads," Times-Picayune (New Orleans). Mrs. Gregson planned to host a series of lectures for civic clubs and older children on the evils of the drug traffic, and called upon concerned citizens to notify her of places where marijuana cigarettes were sold.41For coverage of Gregson's announcement, see "Marijuana War Is Planned by Mrs. Gregson," 9; "No Man's Land," Times-Picayune (New Orleans), December 14, 1924, sec. Three, 15.
The Louisiana Board of Health called upon Dr. Carleton Simon, a narcotic expert, deputy police commissioner, and lecturer on criminology in New York, to conduct a survey of drug use in the state. Simon's investigation concluded that, "thousands of young men and women in Louisiana are addicted to the use of marijuana, known in underworld haunts as 'muggles' and 'moota.'"42"Thousands of State's Youth Marijuana Addicts, Survey by Criminologist Show," Times-Picayune (New Orleans), August 12, 1926, 6. School officials and parent groups reaffirmed Simon's assessment.43For examples, see "Women to Probe Drivers' License Issuance System," Times-Picayune (New Orleans), October 26, 1926, 3; "National Officer of School Clubs Will Visit," Times-Picayune (New Orleans), October 28, 1926, 5; "Public School Vice Quiz Opens Feb. 23," Times-Picayune (New Orleans), February 20, 1927; "School Alliance Holds Meeting—Stricter Legislation Towards Marijuana Sellers Is Urged," Times-Picayune (New Orleans), May 10, 1927; "School Children Smoke Muggles, Alliance Is Told—Startling Reports Made at Meeting by Mrs. J.G. Skinner," Times-Picayune (New Orleans), May 13, 1928. In January 1927, A. H. Seward, president of the Public School Alliance (PSA), charged that marijuana was "being sold to children in the grammar and high schools."44"Gambling in City Leaves Its Mark on School Boys," Times-Picayune (New Orleans), January 11, 1927, 2. By November, the PSA reported, "a slight increase in the number of marijuana, or 'muggles,' cigarettes sold to and smoked by grammar school children." Some of those children were "as young as those of the fourth and fifth grades" with "traces of this habit . . . seen as early as the third grade."45"More Children Smoke Muggles Alliance Hears," Times-Picayune (New Orleans), November 15, 1927, 2.
![Black newspaper-style text on a white background that reads, "(Sample--Warning card to be placed in R. R. Trains, Buses, Street Cars, etc.) Beware! Young and Old — People in All Walks of Life! This [image of marijuana joint] may be handed to you [image of smiling man and woman] by the friendly stranger. It contains the Killer Drug 'Marihuana' — a powerful narcotic in which lurks Murder! Insanity! Death! [Image of marijuana plant] WARNING! Dope peddlers are shrewd! They may put some of this drug in the [image of teapot] or in the cocktail or in the tobacco cigarette. Write for detailed information, enclosing 12 cents in postage—mailing cost. Address: The Inter-State Narcotic Association (incorporated not for profit) 53 W. Jackson Blvd. Chicago, Illinois, U. S. A."](https://southernspaces.ecdsdev.org/wp-content/uploads/2019/07/rathge_005_psa.jpg "Marijuana Warning Poster, ca. 1971. Poster by Inter-State Narcotics Association. Courtesy of the Wisconsin Historical Society.")
The PSA findings resulted in renewed calls for federal intervention.46Their efforts mirrored earlier attempts out of New Orleans urging federal action on marijuana, dating to Dr. Dowling's letters in 1920. For additional examples, see "We Want Walmsley for Congress," Times-Picayune (New Orleans), March 23, 1924, sec. One-B; "Women Endorse City Bond Issue—Federation of Clubs Will Ask Us Action Against Marijuana," Times-Picayune (New Orleans), November 23, 1926, 19. On the Public School Alliance, see "Alliance Seeks Government Ban on Marihuana," Times-Picayune (New Orleans), December 12, 1928, 37. In December 1928, W.O. Hart, PSA legislative committee chairman, began working with Louisiana Representatives James Z. Spearing and James O'Connor to amend the existing federal Harrison Narcotic Act to include marijuana.47The Harrison Narcotics Act of 1914 regulated and taxed the production, importation, and distribution of opiates and coca products as well as closely monitored the proscribing habits of registered physicians. Congressman Spearing was a longtime member, and two-time president, of the Orleans Parish School Board as well as a member of the Louisiana State Board of Education. "Despite the efforts of the alliance and of its private investigators," declared PSA president A. H. Seward, the traffic in this social leprosy still goes on" and would until Congress passed "suitable legislation, laws with teeth in them."48"Children Smoke Marihuana, Says Head of Alliance—Fight for More Severe Legislation to Be Carried On," Times-Picayune (New Orleans), January 15, 1929, 12; "Alliance Seeks Government Ban on Marihuana," 37. That New Orleans played a central role in raising the issue made news as far away as New York—where headlines seized on the city's "fight to save school children."49"War on Hashish Smoking Is Carried to Congress in Effort to Save School Children," The Brooklyn Eagle, December 20, 1928, 3; "Federal Agents Powerless to End Hashish Traffic," The Brooklyn Eagle, December 21, 1928.
The existence of Mrs. Gregson's "marijuana war," the efforts of civic clubs and the PSA, as well as consistent police enforcement demonstrate that prohibitory marijuana laws in New Orleans remained anything but "dormant."50See Bonnie and Whitebread, The Marijuana Conviction, 44. According to Bonnie and Whitebread, in the fall of 1926, New Orleans police suddenly "arrested more than 150 persons for violation of a law which had lain dormant for two years." It is unclear if they mean the city ordinance or the state law. Nevertheless, given the evidence shown here, there was obviously significant attention focused on marijuana for at least four to six years prior to that particular enforcement sweep in 1926. Contemporary reports clearly show continued enforcement and arrests for marijuana under both the city ordinance and state law throughout this period. There was significant and consistent activity aimed at curbing marijuana use in the city beginning in the early 1920s. For the period between June 1923 and December 1929—roughly the first seven years of enforcement for the city's ordinance—reporting from the Times-Picayune highlighted 225 documented marijuana arrests. The paper's reports shed light on the activities of law enforcement as well as the spatial and demographic characteristics of those arrested. Measuring the prevalence of marijuana use in New Orleans during this period remains difficult given the many source biases and limitations surrounding illicit substances. Examining these reports, however, reveals a user population with characteristics different from those often described by contemporary commentary and subsequent historical studies.
Marijuana Users in Time and Place
One of the most striking differences between the newspaper evidence and the existing historiography on marijuana prohibition is the size of the marijuana market. Most historical studies have suggested marijuana use in the 1920s was a highly regionalized, marginal practice confined to Mexican immigrants and fringe groups and likely exaggerated by contemporary sources.51For examples, see Musto, The American Disease; Bonnie and Whitebread, The Marihuana Conviction; John Helmer and Thomas Vietorisz, Drug Use, the Labor Market and Class Conflict (Washington: Drug Abuse Council, 1974); John F. Galliher and Allynn Walker, "The Puzzle of the Social Origins of the Marihuana Tax Act of 1937," Social Problems 24, no. 3 (1977): 367–76; Himmelstein, The Strange Career of Marihuana. The available evidence from New Orleans suggests otherwise.52The widespread digitization of newspapers and related online databases has undoubtedly made this evidence more accessible to researchers and reinforces the need to reevaluate earlier interpretations. Police activity in the city yielded arrests for possession of a single marijuana cigarette to seizures as large as forty pounds. In 1922, the Times-Picayune recorded three raids netting large quantities. In August, police raided the apartment of Genara Prugillo and Lorenzo Espinoza capturing twenty-one gallons of wine and one hundred and ninety packets of marijuana.53"Police Capture Weed, Wine and Owners in Raid," Times-Picayune (New Orleans). A month later customs officials searched a Mexican steamship moored in New Orleans and seized "two large packages of Mexican Marijuana leaves" valued at New Orleans retail prices exceeding $800.54"Narcotic Leaves Seized on Vessel," Times-Picayune (New Orleans). In December, New Orleans police and federal agents completed an undercover investigation they believed would "smash" a local "narcotic ring." The alleged ringleader was captured with "more than $9,000 of cocaine, morphine and mariahuana."55"Drug Ring Hunt Seems to Score," Times-Picayune (New Orleans). Little more than a year later, New Orleans police made a series of arrests that netted similarly large amounts of marijuana, including seizures of fifteen pounds, five pounds, forty pounds, and ten pounds.56"Marihuana Haul Made By Police," Times-Picayune (New Orleans), January 17, 1924; "American Craze for Marihuana Builds Industry," Times-Picayune (New Orleans), March 10, 1924; "Arrest Marihuana Seller," Times-Picayune (New Orleans), March 10, 1924, 14; "Marijuana Seized Valued at $3,000," Times-Picayune (New Orleans), April 20, 1924, sec. Five, 8; "Decision Upholds Recorder's Stand," Times-Picayune (New Orleans), May 1, 1924; "Alleged Ex-Convict Held, Drug Seized," Times-Picayune (New Orleans), May 31, 1924, 3.
Given such volume, it is hard to dismiss the situation in New Orleans as journalistic sensationalism or law enforcement propaganda although it is easy to criticize the contemporary assessment of the dangers posed by marijuana use given our present understanding. The size and frequency of seizures in New Orleans during the early 1920s attest to the scope of the city's marijuana market. Arrests for simple possession as well as large quantities occurred regularly. Street-level arrests and sting operations often yielded only a few marijuana cigarettes, while quantities seized at larger busts ranged from hundreds of pre-rolled cigarettes to many pounds of bulk marijuana.57For examples of large marijuana seizures, see "Woman Charged Under Drug Act," Times-Picayune (New Orleans), September 27, 1924, 2; "Marijuana Seized," Times-Picayune (New Orleans), July 17, 1925, 23; "Liquors and Drugs Seized by Agents," Times-Picayune (New Orleans), March 23, 1926; "Healy Launches Attack on Vice and Marihuana," Times-Picayune (New Orleans), October 17, 1926; "Marijuana Leads to Arrest of Four," Times-Picayune (New Orleans), January 16, 1927; "Marijuana Drugs Are Seized on Ship," Times-Picayune (New Orleans), February 10, 1927, sec. Part Two; "Woman Is Accused of Marijuana Sale," Times-Picayune (New Orleans), June 28, 1927, sec. Part Two; "Two Marijuana Loads Confiscated," Times-Picayune (New Orleans), October 8, 1927; "Agents on Trail of Large Liquor Smuggling Ring," Times-Picayune (New Orleans), November 11, 1927; "Marihuana, Rum Seized by Federal Officers on Ships," Times-Picayune (New Orleans), February 10, 1928; "$5000 in Marihuana Taken from Ship," Times-Picayune (New Orleans), February 29, 1928; "Marihuana Seized by Captain at Sea," Times-Picayune (New Orleans), March 22, 1929; "Customs Agents Seize Marihuana Valued at $7500," Times-Picayune (New Orleans), October 4, 1929, sec. Part Two. These stories signal a market environment with both large-scale peddlers and small quantity buyers.
The evidence also hints at the existence of a subset of repeat offenders. During the city's "first marihuana raids," for example, police arrested Antonio Bernade and his wife—owners of the Black Cat Restaurant—with "twelve packs of the weed."58"Cops Make First Marihuana Raids," Times-Picayune (New Orleans). Just a week later in a second restaurant raid, police arrested Bernade again, finding marijuana "concealed in a false window."59"Alleged Marihuana Seized," Times-Picayune (New Orleans), June 24, 1923. Less than a month later, police alleged that Mrs. Bernade absconded with the marijuana as officers arrived. Mr. Bernade was arrested a third time on charges of selling marijuana cigarettes to Dominick Potania—"a member of one of New Orleans' best families"—as Potania was leaving the restaurant, giving them reason enough to enter.60"Restaurant Man Sold Marihuana, Police Charge," Times-Picayune (New Orleans), July 8, 1923, 9. A report for this arrest gave a different restaurant address and a slightly differently spelling of his name—Antonio Bernabe. Potania seems to have continued his involvement in the illicit drug market. Six years later, a newspaper report chronicled his arrest alongside Carlo Giacona. According to police, Potania "attempted to conceal a packet of cocaine" while Giacona was "alleged to have had a marihuana cigarette."61"Cocaine, Marihuana Found, Two Jailed," Times-Picayune (New Orleans), May 24, 1929. Giacona was ultimately not tried for this offense, see "Records of the Day—Criminal Court," Times-Picayune (New Orleans), June 15, 1929. Two months later police arrested Giacona again following a raid on his boarding room, where detectives reportedly found "a pound of marihuana seeds."62"Police Nab Youth, Seize Marihuana," Times-Picayune (New Orleans), August 1, 1929. Another repeat offender, Sam Farace, faced criminal charges following his arrest with "a pillow slip containing ten pounds of raw marihuana weed." Just out of state prison, Farace was the proprietor of a "soft drink establishment" that city officials alleged was "a rendezvous for thieves and police characters."63"Alleged Ex-Convict Held, Drug Seized," Times-Picayune (New Orleans), 3. Three years later, during a raid on his family's restaurant, police arrested Farace's younger brother Joseph with two dozen marijuana cigarettes. During that incident, Sam Farace reportedly interfered with the police operation and was "arrested, and charged with disturbing the peace."64"Youth Is Taken in Marijuana Raid," Times-Picayune (New Orleans), April 3, 1927, 15.
The presence of repeat offenders suggests a substantial market for the drug with significant financial incentives. Both offenders and those pushing for stiffer penalties raised the idea that penalties for violation of the city's marijuana ordinance were too weak.65For examples, see "A Yarn of Many Threads," Times-Picayune (New Orleans); "Marihuana Peddler Fined," Times-Picayune (New Orleans), July 3, 1923; "American Craze for Marihuana Builds Industry," Times-Picayune (New Orleans); "Arrest Marihuana Seller," Times-Picayune (New Orleans), 14. Valdo Santos spoke with Times-Picayune reporters following his first arrest on marijuana charges and claimed, "It's not hard to get through. Most of it comes overland, through Texas. We pack it in a suitcase and when we sell out we go back for more. It's easy and a good business. Beats bootlegging and the fines are smaller."66"American Craze for Marihuana Builds Industry." For Santos, this apparently meant big rewards and small consequences. He was arrested again a year later with five pounds of marijuana and forty-eight pre-rolled cigarettes.67"Arrest Marihuana Seller," 14. Police Detective Henry Asset agreed that the punishments for marijuana were not a major deterrent and believed violators easily managed to pay the $25 fine. "Any good peddler," he argued, "can raise that amount."68"A Yarn of Many Threads."


Evidence from the Times-Picayune offers some sense of the diversity of people, places, and situations involved in marijuana arrests. Police regularly targeted soft drink stands, groceries, and restaurants and often implicated them as sites of illicit activity, including the smoking and selling of marijuana.69"Liquor and Mary Warner Seized," Times-Picayune (New Orleans), June 5, 1924, 26. In April 1924, for instance, following an undercover purchase at the restaurant of Manuel Arredondo, New Orleans police confiscated some forty pounds of marijuana. Valued at nearly $3,000, the stash was "concealed in the rear of the place under a trapdoor."70"Marijuana Seized Valued at $3,000," Times-Picayune (New Orleans), 8. Police frequently made marijuana arrests on the streets and sidewalks, including eight young men found smoking in Coliseum Square.71For this instance and others, see "Alleged 'Muggles' Habitues Are Fined," Times-Picayune (New Orleans), July 29, 1923, 3; "More Patrolmen Are Transferred," Times-Picayune (New Orleans), September 10, 1923, 13; "Finds Marihuana in Martina's Store," Times-Picayune (New Orleans), October 17, 1923, 7. Though reports suggest police arrested men far more often, there were also female marijuana peddlers arrested.72The roles women have played in the business of drug trafficking is highly understudied. See Elaine Carey, Women Drug Traffickers: Mules, Bosses, and Organized Crime (Albuquerque: University of New Mexico Press, 2014). Mrs. Carrie O'Donnell was in her grocery store and place of residence when police "found thirty-seven marijuana cigarettes, which complainants said she kept for sale."73"Unable to Find Verboten Law," Times-Picayune (New Orleans), October 2, 1924, 7. Police arrested Mrs. Sadie Garden at home where detectives seized "several thousand marijuana cigarettes, bulk marijuana, a box of morphine and a quantity of grain alcohol."74"Woman Charged Under Drug Act," Times-Picayune (New Orleans), 2. In an era of alcohol prohibition, police frequently seized marijuana alongside liquor.75For just one example, see "Possession Is Charged," Times-Picayune (New Orleans), July 30, 1925, 16.
Reporting also linked marijuana seizures to the city's many ships and sailors. Often, federal customs agents were involved in these incidents. Though the Harrison Narcotic Act did not cover marijuana, a 1915 Treasury Decision banned the importation of cannabis if intended for other than medical purposes.76W. G. McAdoo, Treasury Decisions Under Customs and Other Laws, vol. 29 (Washington, D.C.: U.S. Government Printing Office, 1916), 257. In early 1925, two Mexican seamen faced marijuana charges. Police arrested Antonio Corres on the city docks with "a bag containing marijuana."77"Smuggler Sentenced," Times-Picayune (New Orleans), March 5, 1925, 12. In a separate incident, a customs official trailed Manual Gonzalez as he left the steamship Yuma, leading to his arrest for "possessing six pounds of marijuana."78"Marijuana Seized," Times-Picayune (New Orleans), 23. In a third incident, Juan Horgoros, a "Spanish Seaman," faced marijuana possession charges following his arrest by a customs official.79"Spanish Seaman Held," Times-Picayune (New Orleans), October 21, 1925, sec. Part Two, 17. Four years later, customs agents apprehended William Shanakan and Edward Busamente near the Desire street docks as "the pair attempted to land a small skiff underneath the wharf apron and smuggle ashore seven bags of marihuana." The two men obtained the drug from "unnamed members of the crew of the Honduran steamship Baja California." Shanakan and Busamente floated "with the current alongside the ship on the river side and the bags of the hasheesh weed had been let down from a port-hole to the skiff." Since customs agents could not implicate individual crewmembers, they levied a fine on the entire steamship for "unmanifested contraband."80"Pair Arrested Trying to Land with Marihuana," Times-Picayune (New Orleans), October 10, 1929, 1. Given the regularity with which police and customs agents seized large quantities of marijuana from ships and sailors, it appears the city's market for the drug was substantial and frequently supplied by boat.
Some of these arrests and large-scale smuggling cases lend credence to the belief that Mexican immigrants were responsible for bringing marijuana to the United States and that they made up a significant portion of users. The notion that marijuana use was "a casual adjunct to life" for many Mexican immigrants in the early twentieth century has gone virtually undisputed in the historiography on marijuana prohibition.81For the use of this phrase, see Bonnie and Whitebread, The Marijuana Conviction, 33–34. This broad narrative argues that immigrant Mexican laborers brought marijuana smoking into the United States where it spread to local populations in Texas, California, Colorado, and other states west of the Mississippi River.82Generally known as the "Mexican Hypothesis" or the "Mexican Vector model," this is the most prominent interpretation for marijuana prohibition in the United States. For more on these terms, see Himmelstein, The Strange Career of Marihuana; Campos, Home Grown. In this interpretation, anti-Mexican sentiment and blatant racism provided the impetus for many state and municipal level laws prohibiting marijuana. Recently this interpretation has faced a significant challenge. Historian Isaac Campos has shown that marijuana use in Mexico was anything but a regular habit of everyday life and was largely confined to soldiers, prisoners, and other marginalized groups. Most of the general population avoided the drug, believing it caused "madness, violence, and mayhem." Campos argues that rather than bringing marijuana smoking to the United States, Mexican immigrants relayed the idea that marijuana was an incredibly dangerous drug—"one that triggered sudden paroxysms of delirious violence."83Campos, Home Grown, 2, 5.
Contemporary newspaper coverage in New Orleans reveals evidence for many of these interpretations, but yields limited support for widespread use by Mexican immigrants. Rather, a small number appear disproportionately tied to the early distribution network. Many of the largest seizures of marijuana in the city had connections to steamships from Mexico. There were also reports of a few large seizures involving Mexican suspects and false-bottomed suitcases, neatly built for concealing drugs.84For examples, see "Seven Arrested and 36,000 Grains of Dope Seized," Times-Picayune (New Orleans), June 8, 1923; "Dope Swindle Exposed by Raid on Mexican Club," Times-Picayune (New Orleans), June 9, 1923; "Marihuana Haul Made By Police"; "American Craze for Marihuana Builds Industry," Times-Picayune (New Orleans); "Arrest Marihuana Seller," Times-Picayune (New Orleans), 14. Yet, of the 225 documented marijuana arrests in the Times-Picayune between 1923 and 1929, the newspaper identified only thirty-three total suspects by their ethnicity or race. Mexicans accounted for eleven of that thirty-three, and seven of those eleven came from a single seizure. The paper also identified two additional suspects of "Spanish" origin. Another nineteen suspects not explicitly identified by race or ethnicity did have a traditional Mexican or Spanish surname.85These names include: Martinez (five suspects) with one possible repeat offender, Gonzales (two suspects), Mendoza (two suspects), Busamente (one suspect), Rodrigues (one suspect), Ruiz (one suspect), Garcia (one suspect), Lopez (one suspect), Campos (one suspect), Belasques (one suspect), Torres (one suspect), Spinoza (one suspect), and Santos (one suspect). Those specifically identified as Mexican or Spanish by the Times-Picayune accounted for just five percent of the arrests reported between 1923 and 1929. Adding those with traditional surnames, but unidentified by race or ethnicity, yields twelve percent of documented arrests. The 1930 census data shows 717 citizens in New Orleans listed as "Mexican"—accounting for 0.1 percent of the city's 458,762 residents.
The arrival of Mexican immigrants smoking marijuana did not capture the attention of civic groups and law enforcement, nor did the Times-Picayune give much attention to marijuana use by Mexicans. Neither was anti-Mexican or racist sentiment central to the discussion of the New Orleans city ordinance or state law prohibiting marijuana. Given the city's prominence in launching the "marijuana menace" as a nationwide phenomenon, the absence of blatant anti-Mexican sentiment and the limited number of arrests undermines the intense emphasis on Mexican immigrants found in many histories of marijuana prohibition.86For the most prominent examples of the "Mexican Hypothesis," see Musto, "The Marihuana Tax Act of 1937"; Musto, The American Disease; Bonnie and Whitebread, The Marihuana Conviction.

The same was true of African Americans—another group often associated with marijuana use during this period. Bonnie and Whitebread, for example, suggested that the main users of marijuana in New Orleans were "black and lower-class white elements."87 Bonnie and Whitebread, The Marijuana Conviction, 92. Likewise, in the mid-1930s, FBN Commissioner Harry J. Anslinger often proclaimed a connection between marijuana and black jazz musicians. There is indeed little doubt that marijuana played an influential role in the lives and artistry of many jazz musicians by the 1930s, as many popular songs eluded to marijuana in both implicit and explicit ways.88Bob Beach, "'That Funny, Funny Reefer Man': Reading Reefer Madness Through Jazz Music During the 1930s," Points: The Blog of the Alcohol & Drugs History Society, April 30, 2015, https://pointsadhsblog.wordpress.com/2015/04/30/that-funny-funny-reefer-man-reading-reefer-madness-through-jazz-music-during-the-1930s/. Yet, the arrest records featured in the Times-Picayune include almost no references to jazz musicians or African American marijuana users. Between 1923 and 1929, the paper explicitly identified just sixteen suspects as "negro."89This number accounts for about seven percent of the total arrests covered in this article. According to the U.S. Census Bureau, African Americans made up between 26 and 28 percent of the total population of New Orleans. For census data, see Campbell Gibson and Kay Jung, "Historical Census Statistics on Population Totals by Race, 1790 to 1990, and by Hispanic Origin, 1970 to 1990, for Large Cities and Other Urban Places in the United States" (Washington, D. C.: U.S. Census Bureau, 2005), https://www.census.gov/population/www/documentation/twps0076/twps0076.pdf. In the cradle of jazz, during a period defined by the use of racialized terms to distinguish and denigrate African Americans, the local newspaper evidence reveals little connection between these groups and marijuana use.
The lack of African Americans identified among those arrested for marijuana during this period appears especially stark given that the majority of those arrests occurred in and around today's French Quarter.90It is possible that newspaper reports from these areas simply implied the suspects were African American. That seems unlikely, however, given the frequent use of terms like "colored" and "negro" in other reporting by the paper, crime-related or otherwise. The nearby Storyville, Tango Belt, and Back o' Town neighborhoods were home to many African Americans and were prominently associated with vice, entertainment, and jazz. Storyville was the legendary tenderloin district, a sanctioned site of prostitution until 1917. At its peak, the Tango Belt housed one of the highest concentrations of commercial jazz venues in the city. The Back o' Town was the boyhood home of Louis Armstrong and known as the "colored red-light district."91The adjacent South Rampart Street corridor also had many African American businesses. See "Jazz Neighborhoods—New Orleans Jazz National Historical Park (U.S. National Park Service)," accessed September 4, 2016, https://www.nps.gov/jazz/learn/historyculture/jazz-map.htm. Armstrong left New Orleans in 1922, but apparently did not begin using marijuana until white musicians introduced him to the drug in Chicago later that decade. Armstrong was highly fond of marijuana; he recorded the song "Muggles" in 1928, faced jail time in 1930 for marijuana possession in Los Angeles, and reportedly smoked daily for most of his life. For more on Armstrong and marijuana, see Thomas David Brothers, Louis Armstrong, Master of Modernism (W. W. Norton & Company, 2014). Nevertheless, very few of the documented marijuana arrests in these areas identified jazz musicians or African Americans as the suspects. In May of 1925, for example, a Times-Picayune headline proclaimed, "Vice Squad Again Hits Tango Belt; Score Arrested." Of the fourteen men and six women arrested, only two faced marijuana charges, and neither was identified by the paper as African American.92"Vice Squad Again Hits Tango Belt," Times-Picayune (New Orleans), May 16, 1925.

Though most marijuana arrests occurred near North Rampart Street between Elysian Fields Avenue and Canal Street, there were also smaller pockets of arrests throughout the city, especially south of St. Charles Avenue along the Mississippi River. Interestingly, however, the available home addresses for marijuana suspects show a more even distribution throughout the city when compared with their arrest location. This was true of suspects from working-class areas nearer to the river, especially between Magazine Street and Tchoupitoulas Street, as well as suspects from more affluent areas of the city, including the Garden District and the Uptown/Carrollton area near Tulane University. Based on newspaper reports, the average distance between place of arrest and place of residence was 1.7 miles, with a median distance of 1.1 miles.93Distance data was drawn from 115 records that provided an address for both place of arrest and place of residence. Excluding records where the arrest and residence locations were the same, difficult to locate on a current map, or far outside New Orleans (Biloxi, MS, for example), left seventy-seven records for further analysis. Of those records, the average distance from arrest location to their residence was 1.7 miles, with a median distance of 1.1 miles. The maximum distance was 6.8 miles, the minimum less than 0.1 miles, with a mode of 0.3 miles. These patterns of arrest and home address suggest an illicit market, not unlike those of the present, where the sale of illicit drugs is often concentrated in specific areas of the city, but users regularly come from other neighborhoods to buy.
The dearth of documented arrests for African Americans and Mexicans in New Orleans during the 1920s calls into question long-held historiographic beliefs about the demographics of typical marijuana users.94Though it is difficult to draw firm conclusions, based on the available newspaper evidence it is likely that the vast majority of marijuana suspects were white. Contemporary newspapers generally identified non-whites as "Negro," "Colored," "Mexican," or other similar terms. Thus, when the paper did not provide a race or ethnicity, it seems likely the suspect was white. For another example of identifying and classifying race among arrest records in New Orleans, see Tanya Marie Sanchez, "The Feminine Side of Bootlegging," Louisiana History: The Journal of the Louisiana Historical Association 41, no. 4 (2000): 403–33. Indeed, the available arrest evidence from the Times-Picayune suggests the most common marijuana user in the city was a white male in his early twenties.95About 100 of the 225 documented arrests covered in this essay provided the age of the suspect. Of those with a reported age, the average age was 23.5 years old and the median age was 22.5 years old. Evidence from the Times-Picayune also sheds light on the contemporary concern with the use of marijuana by school age children. The belief that New Orleans youth were falling victim to the marijuana habit was a significant factor in the city's sustained efforts at prohibiting the drug and curbing its use. School officials and civic groups repeatedly claimed that children as young as third and fourth grade used marijuana.96For examples, see "Children Using 'Mary Warner,' Officials Fear"; "Gambling in City Leaves Its Mark on School Boys"; "More Children Smoke Muggles Alliance Hears"; "School Alliance Holds Meeting—Stricter Legislation Towards Marijuana Sellers Is Urged"; "School Children Smoke Muggles, Alliance Is Told—Startling Reports Made at Meeting by Mrs. J.G. Skinner"; "War on Hashish Smoking Is Carried to Congress in Effort to Save School Children"; "Children Smoke Marihuana, Says Head of Alliance—Fight for More Severe Legislation to Be Carried On." Despite the fact that little more than anecdotes supported these assertions, newspaper arrest reports do offer some clues. Of the approximately one hundred arrest reports that provided an age, some twenty-five percent were teenagers. Sixty percent were in their twenties, most under the age of twenty-four. The youngest documented arrest in the Times-Picayune was sixteen-year-old William Casey, seized alongside three other men in their twenties "smoking marijuana cigarettes in the rear room of a soft-drink shop."97"Marijuana Leads to Arrest of Four," Times-Picayune (New Orleans). Two police officers arrested seventeen-year-old Eddie Barker with marijuana cigarettes after he nervously ran away when they approached him on the sidewalk.98"Youth Is Arrested," Times-Picayune (New Orleans), January 15, 1929. Though it is difficult to draw sweeping conclusions from such limited data, there is nonetheless enough evidence here to support insight into the city's concern with youthful marijuana use.
Conclusion: Patterns and Precedents from the Big Easy
As one of the first significant metropolitan markets for marijuana, New Orleans offers fascinating insights into the user population and an excellent test case for existing historiography. Based on newspaper evidence there is little doubt that a thriving illicit market for marijuana existed throughout the 1920s and continued long into the 1930s, as arrests for violation of city and state ordinances continued apace. So, too, did a stern resolve among numerous civic groups, local officials, and law enforcement to curb marijuana use.99For an excellent contemporary summary of various high points in the New Orleans anti-marijuana campaign during the 1920s, see "Crime Trail Widens as Marihuana Fume Descends Upon City," Times-Picayune (New Orleans), April 21, 1929, 22, 24. New Orleans played an outsized role as the "hypodermic needle feeding the entire Middle West with drugs" and as a clear nexus of the "marijuana menace" paradigm.100"Port Termed Hypodemic Needle Feeding Entire Middle West with Drugs," Times-Picayune (New Orleans), March 6, 1926, 1. Locally, two common themes informed the characterization of marijuana as dangerous—a link between the plant and crime alongside a perceived threat to its growing use by young people. The existing historiography offers minimal city- or state-level research on marijuana markets during these years, often dismissing claims of rising use as sensational journalism, police propaganda, and xenophobia. Previous studies have often perpetuated the belief that marijuana use was most prominent among African American musicians and Mexican immigrants, which prompted a racist backlash against the drug that led to its criminalization.101See Himmelstein, "The Rise of the Killer Weed," in The Strange Career of Marihuana, 49–75. Though subsequent scholars have largely ignored his conclusions, Jerome Himmelstein remains a notable exception to this dominant interpretation. In 1983, Himmelstein emphasized the importance of youthful marijuana use in prompting federal action on marijuana in the mid-1930s. Though this essay lends credence to that finding, it also shows the specter of marijuana use among children originated in New Orleans more than a decade earlier. Without discounting the role of overt racism in early marijuana legislation across the United States, the evidence from New Orleans shows a more complicated picture as the demographic and spatial nature of the city's marijuana market contrasts with those common depictions in the existing literature.
New Orleans is perhaps the best place in the United States to witness the emergence and consolidation of anti-marijuana sentiment, serving as the epicenter for what became broadly known as the "marijuana menace." Events that transpired in the Big Easy during the 1920s and 1930s influenced and previewed what emerged at the federal level. The ways in which media coverage, law enforcement, and civic concerns in New Orleans coalesced and reinforced a negative characterization of marijuana repeated themselves elsewhere across the country. The city's concern with youthful marijuana use and the drug's alleged criminogenic effects proved highly influential in the push for federal marijuana legislation. New Orleans produced a tight coterie of local law enforcement, public health, and social welfare officials who carried their anti-marijuana campaign to the federal level. So much so that when Commissioner Anslinger and the FBN launched the now infamous "reefer madness" campaign in the mid-1930s, they drew on existing depictions of marijuana gathered from sources across the country—especially the "muggleheads" of New Orleans.
Acknowledgments
Many thanks to Southern Spaces staff members Stephanie Bryan, who helped create the digital maps published here, and Hannah C. Griggs, who copyedited the map database spreadsheets.
About the Author
Adam R. Rathge holds a PhD in American history from Boston College. His dissertation and book manuscript, "Cannabis Cures: American Medicine, Mexican Marijuana, and the Origins of the War on Weed, 1840–1937," charts nearly a century of medical discourse, social concern, and legislative restrictions surrounding the drug, demonstrating that the origins of our nation's prohibitions on marijuana are much older and more complicated than previous studies have suggested. He is currently Director of Enrollment Strategies at the University of Dayton, where he also teaches undergraduate courses as part-time faculty in the department of history.
]]>Introduction

In the winter of 1936, Minnie Lee Ishcomer left home in Idabel, Oklahoma, and journeyed to Hot Springs, Arkansas. Thirty years old, white, poor, and the victim of a long-standing venereal infection, Ishcomer came to Hot Springs hoping to obtain treatment at the VD clinic operated there by the United States Public Health Service (PHS). Her experience was less than satisfactory. Because the clinic officially admitted only acute, infectious VD cases, Ishcomer was initially denied entrance—on the grounds that she was "not a danger to the public health." She passed her first few days in Hot Springs in search of food and shelter. Without money, she made her way to a bus station where a police officer found her "in a very serious condition." Taken back to the clinic, she received a few days' treatment. Soon after her release, a PHS official angrily wired the health officer in Ishcomer's home county that "such cases will not be treated in the future."1H.S. Cumming, Surgeon General, to Charles M. Pearce, State Health Commissioner, Oklahoma, January 29, 1936, General Records of the Venereal Disease Division, 1918–1936, 203.4, in RG 90, Records of the Public Health Service, 1912–1968, National Archives, College Park, Maryland. Hereafter VD Division Records.
The treatment Minnie Lee Ishcomer received likely did little to improve her health.2Available federal census information indicates that in 1930, Ishcomer was married and had a least one son. Her husband appears to have been a mill hand but no occupation is listed for her. Exactly which of her conditions triggered resentment by clinic doctors is not clear. Nevertheless, her story sheds light on a relatively unexplored site of public health work in the early twentieth-century US South.3For a brief overview of the Hot Springs VD clinic, see Edwina Walls, "Hot Springs Waters and the Treatment of Venereal Diseases: The U.S. Public Health Service Clinic and Camp Garraday," Journal of the Arkansas Medical Society 91, no. 9 (1995): 430–7. The opening of the Hot Springs VD clinic in 1921 followed upon extensive anti-venereal initiatives carried out by the U.S. military during World War I. Closing in the 1940s, the clinic marked a transition in the federal government's campaign against syphilis and gonorrhea—including the Tuskegee Syphilis Study (1932–72) and the Chicago Syphilis Control Project (1937–40). Throughout the interwar period, Hot Springs sat on the front lines of the PHS's war against VD, and although its efforts were largely unsuccessful, the clinic's history points toward a more complex understanding of this moment of "venereal peril."4The term "venereal peril" was a staple of turn-of-the-century discourse around syphilis and gonorrhea. For a particularly good example of this, see William Leland Holt,The Venereal Peril: A Popular Treatise on the Venereal Diseases, ed. William Josephus Robinson (New York: The Altrurians, 1909). For historical studies on this, see Theodor Rosebury, Microbes and Morals: The Strange Story of Venereal Disease (New York: Viking Press, 1971); Allan Brandt, No Magic Bullet: Venereal Disease and American Society since 1880 (New York: Oxford University Press, 1987); Suzanne Poirier, Chicago's War on Syphilis, 1937–40: The Times, the Trib, and the Clap Doctor (Urbana: University of Illinois Press, 1995); Nancy K. Bristow, Making Men Moral: Social Engineering during the Great War (New York: New York University Press, 1996); Andrea Tone, Devices and Desires: A History of Contraceptives in America (New York: Hill and Wang, 2001); Marilyn Hegarty, Victory Girls, Khaki-Wackies, and Patriotutes: The Regulation of Female Sexuality during World War Two (New York: New York University Press, 2008); John Parascandola, Sex, Sin, and Science: A History of Syphilis in America (Westport, CT: Praeger, 2008).

The history of the Hot Springs clinic offers insights into racial, gendered, and class-based aspects of the federal government's campaign against syphilis and gonorrhea. The clinic treated all manner of patients—black as well as white, male as well as female. Some patients were chronically poor, and others—particularly with the onset of the Great Depression—had only recently fallen on hard times. How similar were the experiences of these different groups, and to what extent did their treatment reflect prejudices against the various "others" (such as prostitutes and African Americans) popularly associated with VD? While many historical VD studies examine population subsets, this article about Hot Springs offers a more comprehensive analysis, comparing the experiences of stigmatized groups along with those of Hot Springs's prototypical health-seekers: syphilitic white males. Although they accounted for the vast majority of the clinic's caseload, white men have not received significant attention in VD historiography. Including their experiences adds new depth to our understanding of the "venereal peril" while illustrating how forcefully eugenics pervaded the PHS's campaigns against syphilis and gonorrhea.
Eugenics, of course, figures prominently in scholarship on the infamous Tuskegee Study. This experiment, in which the PHS deliberately withheld treatment from four hundred syphilitic Alabama black men in order to study the disease's "natural" progression, was designed to provide evidence for the theory that (as the Johns Hopkins syphilologist Joseph Moore put it) "syphilis in the negro is in many respects almost a different disease from syphilis in the white."5Susan Reverby, Examining Tuskegee: The Infamous Syphilis Study and Its Legacy (Chapel Hill: University of North Carolina Press, 2009), 136. From 1932 to 1972 white PHS doctors attempted to prove that black syphilitics almost never progressed to the late, advanced stage of the disease characterized by disorders of the nervous system–including tabes (syphilis of the spinal cord) and paresis (syphilis of the brain). Blacks were seen as belonging to an uncivilized race with smaller, less developed brains that equipped them with a "racial resistance" to neurosyphilis; as a result, they were more likely to suffer from the disease's cardiovascular symptoms—including syphilis of the heart.6Christopher Crenner, "The Tuskegee Syphilis Study and the Scientific Concept of Racial Nervous Resistance," Journal of the History of Medicine and Allied Sciences 67, no. 2 (2012): 244–80. Doctors believed that this partial immunity to neurosyphilis was a hereditary trait. As the authors of a recent article on Tuskegee observe, the experiment's goal was to "prove the biological basis of racial difference by documenting race-linked pathology, consistent with prevailing eugenic theory."7Paul A. Lombardo and Gregory M. Dorr, "Eugenics, Medical Education, and the Public Health Service: Another Perspective on the Tuskegee Syphilis Experiment," Bulletin of the History of Medicine 80, no. 2 (2006): 313.
In providing an assessment of intellectual undercurrents circulating through the PHS in the 1920s and 1930s, this new literature successfully rebuts the claim that Tuskegee had little to do with scientific racism or eugenics.8For a recent article in the revisionist vein, see Thomas G. Benedek and Jonathon Erlen, "The Scientific Environment of the Tuskegee Study of Syphilis, 1920–1960," Perspectives in Biology and Medicine 43, no. 1 (1999): 1–30. Unanswered, however, is how eugenic theories informed aspects of the agency's anti-venereal work involving non-blacks. At Hot Springs, these theories found expression in a campaign designed to prevent the clinic's mostly white male patients from succumbing to the "racial poison" that was VD. Comprising traditional medical services and a variety of extra-medical measures (including financial assistance for food, shelter, and basic care), this campaign cost hundreds of thousands of dollars, with its budget increasing dramatically during the early years of the Great Depression—just as the PHS dismantled a number of pilot projects designed to provide mass treatment to syphilitic blacks. Although many of the initiatives undertaken in Hot Springs benefited patients regardless of race or sex, the clinic's white male health-seekers experienced a level of preferential treatment denied to both women and African Americans. Further, for the latter group, discrimination and hostility were part and parcel of the Hot Springs experience—both inside and outside the clinic. All of this represented the eugenic impulses coursing through the PHS facility, whose director—Oliver C. Wenger—declared syphilis and gonorrhea important "from the standpoint of race conservation."9O.C. Wenger, "The Need for Social Hygiene," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives.
Hot Springs reveals a significant instance of the federal government's racist approach to public health policy. When dealing with white patients, Washington extended a taxpayer-supported hand. Because such a sizable gap existed between the experiences of Hot Springs's black and white health-seekers, the story of the city's VD clinic provides a further context for understanding the Tuskegee Study. But first, a more elementary question: why did the PHS decide to create a VD clinic at Hot Springs, Arkansas?
"Mecca for Syphilitics"
: 251–253.")
Hot Springs's selection as the site of the federal government's "model" VD clinic would not have surprised early twentieth-century Americans.10C.N. Myers, "Hot Springs and the Model Federal Venereal Disease Clinic," Medical Review of Reviews 28 (1922): 86. In 1832, Congress declared that the boiling waters of the Ouachita Mountains were to be forever set aside for the "benefit and enjoyment" of the general public.11For more on the city's early history and the role of the Hot Springs Reservation, see Janis Kent Percefull, Ouachita Springs Region: A Curiosity of Nature (Hot Springs, AR: Ouachita Springs Region Historical Research Center, 2007). In 1877, Congress created the Hot Springs Reservation (HSR). Initially consisting of 2,529 acres, the HSR was public land managed by a federally-appointed commission, whose task was to maintain and control access to the 826,000 gallons of water that daily coursed through the site.12J.K. Haywood, Analyses of the Waters of the Hot Springs of Arkansas (Washington, D.C.: Government Printing Office, 1912), 5. Word of the area's therapeutic prowess spread across the country, and as the city began welcoming hundreds of health-seekers every year, its waters acquired a reputation for curing syphilis.13For evidence of this, see A.J. Wright, "Some Account of the Hot Springs of Arkansas," The New Orleans Medical and Surgical Journal (1860): 798–9, 801; R.M. Lackey, "The Hot Springs of Arkansas," Chicago Medical Journal 23 (1866): 9; J.L. White, "The Hot Springs of Arkansas," Chicago Medical Recorder 36 (1878): 311. During the late nineteenth-century, a growing belief in the springs' ability to "drive out syphilis completely" spurred a "Hot Springs craze" among venereal sufferers. Contemporaries began referring to the city as the "Mecca for syphilitics in America."14S.B. Houts, "Cases in Practice," The Medical World 5 (1887): 248–52; Edward L. Keyes, The Venereal Diseases, Including Stricture of the Male Urethra (New York: William Wood & Company, 1880), 107–8; E.R. Lewis, "The Hot Springs of Arkansas," The Kansas City Medical Index-Lancet 10, no. 7 (1889): 249. For references to Hot Springs as a "Mecca" for syphilitics during the late-nineteenth and early-twentieth centuries, see "Editorial: Syphilis of the Nervous System," The Hot Springs Medical Journal 3, no. 2 (1894): 51; A. Ravogli, "The Thermomineral Cure in the Treatment of Syphilis," The Medical Era 6, no. 8 (1897): 276; Bukk G. Carleton, A Treatise on Urological and Venereal Diseases (New York: Bukk G. Carleton, 1905), 741; Loyd Thompson, Syphilis (Philadelphia, PA: Lea and Febiger, 1920), 212.
While some of Hot Springs's health-seekers received treatment at the Free Government Bathhouse created by the HSR in 1878, increasing numbers did so at private enterprises.15Haywood, Analyses of the Waters, 5. Hot Springs was "fast becoming a fashionable resort."16J.L. Gebhart, "On the Therapy of the Waters of Hot Springs, Arkansas, and Their Relation to the Medical Profession at Large," St. Louis Medical and Surgical Journal 38 (1880): 634. Leasing land and water from the HSR, local developers began replacing the city's "miserable board shanties" with "palatial hotels."17Robert Heriot, "Letter to the Editor," Locomotive Engineers Journal 25 (1891): 919. The resort's clientele shifted: earlier the preserve of "poor, miserable paupers," it was increasingly visited by "very wealthy people from the Northern states."18E.B. Stevens, "Hot Springs, Arkansas," Transactions of the Ohio Medical Society 31 (1875): 197; Heriot, "Letter to the Editor," 919. See also H.M. Rector, "Then and Now," Hot Springs Medical Journal 4 (1895): 225; Henry Durand, "Uncle Sam, M.D., and His Great Sanitarium," The American Monthly Review of Reviews 16 (1897): 75–9. To ensure that its visitors remained a "people of leisure, with an abundance of money to spend," local officials forcibly uprooted the city's poorer health-seekers—those living in "shanties or tents" or found "encamped under the trees with no other shelter."19"Hot Springs, Arkansas," The Medical Visitor 20 (1904): 140; "Hot Springs, Arkansas, as a Health Resort," Hot Springs Medical Journal 3, no. 6 (1894): 173; William H. Deaderick, "The Development of the Hot Springs of Arkansas as a Health Resort," The Medical Pickwick 2 (1916): 265–6. One turn-of-the-century visitor reported on how "it was the policy of the municipality of Hot Springs to discourage the coming of the poor people to that place," which it did "by withholding all of the usual eleemosynary institutions from their use." Hal C. Wyman, "A Surgical Pilgrimage to Arkansas," Physician and Surgeon 28 (1906): 207. Medical authorities in other locales came to believe that "only the rich" could afford the "costly excursion" to Hot Springs.20"Syphilitic Paresis," The Eclectic Medical Journal 50 (1890): 562. As a Chicago physician said of his city's syphilitic patients: "our rich people go to the great Mecca of medical wisdom, to Hot Springs," while "our poor people may go to—where they please."21Joseph Zeisler, "The Social Evil," Year Book (Chicago: The Sunset Club, 1894), 218.


The invention of Salvarsan (1910), a more effective drug, also prompted a decline in the city's voluminous traffic in syphilitic health-seekers.22"Since the arsphenamines have justly become popular," the director of the Hot Springs VD clinic observed in 1921, "the number of syphilitics coming to Hot Springs has been decreased year by year." O.C. Wenger, "The Early Days of Hot Springs, Arkansas (1850–1900)," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives. Nevertheless, neither new drugs nor the discrimination against impoverished health-seekers succeeded in severing the city's association with VD.23"We see every day, here in Hot Springs," one local physician noted in a 1913 treatise, "from ten to a hundred persons" suffering from the "terrible disease" that was syphilis. Albert J. Whitworth and John M. Byrd, The Hot Springs Specialist (Memphis, TN: B.C. Toof & Company, 1913), 164. For more about Salvarsan, see Patricia Spain Ward, "The American Reception of Salvarsan," Journal of the History of Medicine & Allied Sciences 36, no. 1 (1981): 44–62. In 1920, the HSR created a new, expanded Free Government Bathhouse; its lower floor would soon become home to the PHS's VD clinic.24Oliver C. Wenger, "The Early Days in Hot Springs, Arkansas (1850–1900)." Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives. As its director put it upon entering the city that same year: "to the average layman, Hot Springs, Arkansas, means VD, and VD means Hot Springs."25Oliver C. Wenger, "Results of a Study and Investigation of Venereal Disease at the United States Public Health Service Clinic at Hot Springs, Arkansas," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives.
Hot Springs's status as federal land and as a "mecca" for syphilitics made the city an ideal site for the PHS's "model" VD clinic. But why would the government create such a clinic? The early twentieth-century was a time of profound anxiety over syphilis and gonorrhea, diseases said to be "undoubtedly on the increase."26George P. Dale, "Moral Prophylaxis," The American Journal of Nursing 11, no. 9 (1911): 689. It is unknown whether the general prevalence of VD increased during the late nineteenth and early twentieth centuries. What changed was likely not the percentage of the population infected by syphilis or gonorrhea, but instead, the medical profession's awareness of how many illnesses originated in one of these two diseases. Medical authorities proclaimed that 80 percent of adult males living in large cities contracted syphilis or gonorrhea before the age of thirty, and that 80 percent of all operations performed on women for diseases of the womb and ovaries were the result of one of these conditions. Such figures, though highly suspect, engendered fears of a looming VD epidemic across the country.27For these estimates, see G. Shearman Peterkin, "A System of Venereal Prophylaxis That is Producing Results," American Medicine 10 (1906): 328. A colleague named John Cunningham declared that "it is a fact worthy of consideration that every year in this country 770,000 males reach the age of maturity. It may be affirmed that under existing conditions at least 60 percent, or over 450,000 of these young men will sometime during life become infected with venereal disease, if the experience of the past is to be accepted as a criterion of the future." John C. Cunningham, "The Importance of Venereal Disease," The New England Journal of Medicine 168, no. 3 (1913): 77–8.
The sense that venereal diseases constituted "a menace to the national welfare" stemmed less from epidemiology than from social and cultural concerns—of "race suicide" attendant upon the declining fertility of native, white-born women and the influx of "new immigrants," of urbanization and its impact on sexual mores, of a "family crisis" prompted by the emergence of the "new woman," and of eugenic concerns tied to the rhetoric of social Darwinism and racial degeneration.28Abraham L. Wolbarst, "The Venereal Diseases: A Menace to the National Welfare," Medical Review 62 (1913): 327–80. Reformers clamored for an attack on prostitution, artists luridly illustrated the consequences of untreated syphilitic and gonorrheal infections, and anxious legislators passed laws that ranged from the reporting of all professionally-handled VD cases to the bacteriological examination of immigrants and prospective spouses.29For more on this, see Brandt, No Magic Bullet.
The climax of these fears came during World War I. With scientific diagnoses, doctors found that a surprisingly high number of prospective US military recruits suffered from VD. Hoping to head off a manpower shortage, in 1917 Congress created the Committee on Training Camp Activities—an organization that sought to curb the venereal scourge through the forced incarceration of prostitutes, the provision of medical services for infected soldiers, and the establishment of "wholesome" alternatives to the vice-ridden recreational opportunities commonly found in cantonment zones.30See Bristow, Making Men Moral. See also Alexandra M. Lord, "Models of Masculinity: Sex Education, the United States Public Health Service, and the YMCA, 1919–24," Journal of the History of Medicine and Allied Sciences 58, no. 2 (2003): 123–52. The following year Congress passed the Chamberlain-Kahn Act, which created the PHS's Division of Venereal Diseases and allocated two million dollars for the establishment of free VD clinics across the country.31For the Chamberlain-Kahn Act, see Alexandra M. Lord, "'Naturally Clean and Wholesome': Women, Sex Education, and the United States Public Health Service, 1918–1928," Social History of Medicine 17, no. 3 (2004): 423–41. As the war came to a close, Washington followed up on these efforts by conducting a nationwide VD survey.

Each of these actions drew attention to Hot Springs. Throughout the war, military authorities fretted over Little Rock's Camp Pike, a training facility whose VD rates were reportedly "the [highest] by far of any camp or cantonment in the United States."32Victor C. Vaughan, "Protection of American Army Against Social Diseases by More Rigid Health Laws," The Pennsylvania Medical Journal 22 (1918): 26. According to Vaughan, the venereal disease rate at Camp Pike was 568.7 per 1,000 soldiers. See also, "Disease Conditions among Troops in the United States: Extracts from Telegraphic Reports Received in the Office of the Surgeon-General for the Week Ending October 19, 1917," Journal of the American Medical Association 69 (1917): 1535–6; "Venereal Disease and Birth Control," Journal of the Switchmen's Union 20 (1918): 756. According to local commanders, Camp Pike's reputation as a hotbed of sexual sickness owed to its proximity to Hot Springs, where prostitution had been legal since the late nineteenth-century and where brothels enjoyed a reputation as home to the profession's "aristocrats."33For evidence of this, see the letters of Archie C. Cowles, a syphilitic health-seeker who traveled to Hot Springs in 1905. In a letter dated December 10, 1905, Cowles wrote that "many of the women here seem to be on the courtesan order. Of course, it would not do to call them prostitutes," Cowles remarked, "for they are aristocrats in their profession." For Cowles' correspondence, see the Archie C. Cowles Papers, Garland County Historical Society Archives, Hot Springs, Arkansas. In August 1918, Camp Pike's commanders ordered the closure of Hot Springs's numerous "houses of immorality."34"Commissioners Issue Order to the City Manager to Close the Houses of Immorality, Which Goes into Effect at Once," Hot Springs Sentinel-Record, August 2, 1918. Local businessmen and religious leaders rejected the association the military made between Camp Pike's high venereal disease rate and the "terrible conditions" in Hot Springs. See "Ministerial Men to Discuss Morals: Report from Washington of Bad Conditions Here Stirs some Enthusiasts," Hot Springs Sentinel-Record, August 9, 1918; "The Moral Condition," Hot Springs Sentinel-Record, August 10, 1918. Municipal authorities reluctantly complied, but the federal government's interest in Hot Springs did not end. While conducting their post-war VD survey, government officials grew increasingly anxious about the city's "serious medical and social problems," observing that Hot Springs was home to an increasing population of venereally afflicted "indigents" and an entirely "inadequate" public health infrastructure.35Audrey Wenger McCully, "The United States Public Health Service Venereal Disease Clinic and Government Free Bathhouse, 1919–1936," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives.
From the federal perspective, syphilitic health-seekers represented an "interstate menace."36"Proceedings of the Minnesota Academy of Medicine," Minnesota Medicine 5 (1922): 61. The PHS determined to "protect the rest of the country" from those who traversed it with a venereal infection.37First Deficiency Appropriation Bill, 1921; Hearings before Subcommittee of House Committee on Appropriations, 66th Congress, 3rd Session (Washington, D.C.: Government Printing Office, 1921), 588. Opening a clinic in Hot Springs devoted to rendering the afflicted non-infectious seemed the best means of accomplishing this goal. Because patients traveled here from all parts of the country, constituted a diverse racial and socioeconomic makeup, and encompassed the full range of syphilitic infections, the PHS also found in Hot Springs an unprecedented opportunity for research. Establishing a long-term presence here would also allow the government to continue its wartime campaign against "houses of immorality," while transforming a parochial medical culture.38This last point holds for all of the public health campaigns undertaken in the early twentieth-century US South. In the case of Hot Springs, the city was seen as a center of quackery, and in particular, of the country's VD patent medicine industry. See Excluding Advertisements of Cures for Venereal Diseases from the Mails; Hearings before the Committee on the Post Office and Post Roads of the House of Representatives, 66th Congress, 1st Session (Washington, D.C.: Government Printing Office, 1921).

In late 1920 the PHS drew up plans for the facility, obtained $300,000 in construction funds and selected Oliver C. Wenger, one of the country's leading venereologists, as director.39During the war, Wenger—a native of St. Louis—served in the Medical Corps of the Missouri National Guard, and later focused his efforts on "venereal disease prophylaxis" as a member of Sanitary Squad #18, stationed in Camp Mills, a military camp in Long Island, New York. Afterwards, Wenger sought and obtained appointment as a "regional consultant" in the PHS, whereupon he assisted in the nationwide venereal disease survey (1919–20). See McCully, "The United States Public Health Service." Born in St. Louis in 1884, Wenger obtained his MD from St. Louis University in 1908. During the First World War, he served in the Medical Corps of the Missouri National Guard, later traveling to England and France as part of a sanitary squad involved in VD control.40For more on Wenger's biography, see McCully, "The United States Public Health Service." His time in Europe convinced Wenger to devote all his efforts to venereology. According to a contemporary, Wenger's idea of heaven was a place containing "unlimited syphilis," and of course, "unlimited facilities to treat it."41Reverby, Examining Tuskegee, 141. In 1919, Wenger joined the PHS Division of Venereal Disease. Before becoming director at Hot Springs, his first assignment was the national VD survey.
Inside the Clinic

With an inaugural budget of $40,000, the clinic opened in August 1921.42Oliver C. Wenger to C.C. Pierce, March 16, 1921, Hot Springs National Park Administrative Archives, Subseries 25.1.4, File A7615[04]. Hereafter NPS Archives. In its first year, five hundred patients received treatment; a total of 61,930 patients—male and female, black and white—had wound their way through by 1936, receiving 1.2 million injections of mercury and Salvarsan. Who were these individuals? How did their circumstances, needs, and experiences differ? How did prevailing ideas about VD actions influence Hot Springs's response to syphilis? And how did the clinic's campaign develop over the course of the 1920s and 1930s?
On one level, the PHS's day-to-day work reflected the widespread belief that VD constituted the "wages of sin"—a sign of sexual immorality. In lectures given by clinic personnel, patients learned that their illnesses were the result of "ignorance and your own misconduct." This message of personal irresponsibility also extended to the clinic's official instructions, which warned patients not to "loaf downtown" between treatments. Above all other commandments stood one: "DON'T GET INTO TROUBLE." And because the minimum course of therapy lasted between twenty and thirty weeks, patients were "expected to make arrangements to pay [their] own room and board."43Oliver Wenger, "Instructions" (1921), Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives.
Figure 1: VD Cases Admitted to the Hot Springs Clinic, 1922–1936

The PHS advised that "no patient should go to Hot Springs without at least a return ticket and $100 in cash." Such expectations clashed with reality. Wenger observed that "less than five percent of these indigent persons had funds with which to maintain themselves while receiving free treatment."44McCully, "The United States Public Health Service." Many arrived "without one cent of money."45O.C. Wenger, "The United States Public Health Service Clinic at Hot Springs National Park, Arkansas," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives. In 1931, the average applicant carried not "$100 in cash" but $15.43. The following year, $8.76.46Oliver C. Wenger, "A Comparative Study of the Amount of Money Each Applicant Declared Under Oath at the U.S. Government Bath House for the Years 1931–32," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives. Resembling a "dumping ground of many indigents" during the 1920s and 30s, Hot Springs became the preserve of all sorts of "unfortunate people" who "slept out on the hillside or in alleys, begging food from door to door...or looking for food in garbage cans."47 O.C. Wenger, "United States Conducts Clinics for Venereal Diseases," Nation's Health 8 (1926): 103; McCully, "The United States Public Health Service." As the clinic's director admitted, "the great majority left…before they could receive enough treatment to give them any real benefit."48McCully, "The United States Public Health Service."
One of this "great majority" was Virgil Oren Adams. A native of Clovis, New Mexico, during the early 1930s Adams made several visits to the Hot Springs VD clinic. Each time, he "ran out of funds" after only a few weeks, and being "sick and weak from lack of food and sleep," was forced to leave. In 1934 he wrote to President Roosevelt seeking assistance for yet another clinic trip. "I have been fighting syphilis since 1927," Adams wrote, adding that he was "very much interested in…getting rid of this terrible disease." "[A]bsolutely broke," Adams entreated Roosevelt for a letter to take "as a recommendation for treatments at Hot Springs." "Anything you can do in my behalf," he pleaded, would be "highly appreciated."49Virgil Oren Adams to President Franklin D. Roosevelt, September 27, 1934. Part of Adams's story also derives from a letter he sent to Captain Geoffrey, an officer at the Hot Springs clinic. For full texts, see VD Division Records.
Cases like Adams's were of "daily occurrence."50Oliver C. Wenger to the Surgeon General, October 18, 1934, VD Division Records. While poverty hampered patients' chances of recovery, so did the advanced state of their ailments. Most venereal sufferers came to Hot Springs long after contracting syphilis or gonorrhea. Most had not received more than a few shots of mercury or Salvarsan, and many relied only on cheap, ineffective patent medicines.51For evidence of this, consider the case of James Gordon. A Michigan man, in 1926 Gordon wrote the PHS asking for help in getting to Hot Springs. "I have tried [sic] all kinds of medicines, which you know that it [sic] takes money." From a book he had read, Gordon surmised that "there is not mutch [sic] chance for a poor man there," but still he pleaded: Hot Springs was "the last chance I have got—I have every thing [sic] else until my money is gone." For this letter, see James R. Gordon to United States Public Health Service, August 17, 1926, VD Division Records. Their illnesses were chronic, and generally immune to existing remedies. With disease burrowed deep in their bodies, few had any hope of ever being free from VD.

Realities such as these inspired a modicum of sympathy among clinic doctors. Particularly worrying to Wenger was the fate of ex-servicemen. Disappointed by the fact that during World War I, "our young American manhood" was often "unable to serve because of venereal diseases," Wenger observed hundreds of infected former soldiers seeking admittance to the Hot Springs clinic during the early 1920s. Like most patients, they were "nomads, seeking treatment here and there." Particularly troubling was the fact that these veterans were beginning to form families, and had entered "the best years [of their lives] from an economic standpoint." All of them needed medical attention; none were in a position to pay. Such matters made the treatment and control of syphilis and gonorrhea a national priority, he urged, especially "from the standpoint of race conservation."52Wenger, "The Need for Social Hygiene."
Language such as this dovetailed with contemporary eugenic discourse. Like other eugenicists, Wenger's interest in "race conservation" stemmed from anxieties over white racial purity and integrity. Over the course of the nineteenth and early twentieth centuries, birth rates among native-born white women declined by approximately 45 percent, and this, coupled with the simultaneous arrival of millions of "new immigrants" from southern and eastern Europe, prompted fears of "race suicide" among the nation's political and cultural elite.53For more on America's fertility transition, see J. David Hacker, "Rethinking the 'Early' Decline of Marital Fertility in the United States," Demography 40, no. 4 (2003): 605–20. Speaking to these fears, New York City gynecologist Abraham Wolbarst opined that "the flower of our land, the mothers of our future citizenship, are being mutilated and unsexed by surgical life-saving diseases, particularly gonorrhea."54Wolbarst, "The Venereal Diseases," 373. Sentiments such as Wolbarst's were widely held by PHS officials, including Oliver Wenger—whose eugenic beliefs scholars have also observed in his later work in Tuskegee and Chicago.55For more on this, see Reverby, Examining Tuskegee, 139–44.
The PHS sought means of accelerating the therapeutic process. Among the myriad venereological experiments conducted at Hot Springs, none loomed larger than those undertaken within the Salvarsan room. During the early 1920s clinic personnel began "the intensive and continuous plan of treatment."56McCully, "The United States Public Health Service." In the typical VD clinic, patients received one dose of Salvarsan per week; in Hot Springs, they would receive twice that amount.57J.R. Waugh and Elizabeth Milovich, "Severe Reactions to Arsphenamine among 3,050 Previously Untreated Patients," Journal of Venereal Disease Information 21, no. 12 (1940): 391. The Hot Springs clinic, it bears noting, was far from the only site where this experimental use of Salvarsan took place. In the medical literature of the time, many physicians reported success with an accelerated treatment regimen, and some recommended giving as many as three doses in a twenty-four hour period. One advocate advised colleagues to "give the largest possible amount of salvarsan in the shortest possible time." Faxton E. Gardner, "The Treatment of Syphilis," Medical Times 45 (1917): 63. For more discussions of the intensive and continuous treatment of syphilis with Salvarsan, see Frederick W. Smith, "The Modern Diagnosis and Treatment of Syphilis," Medical Record 91 (1919): 186–91; B.C. Corbus, "Prophylaxis in Cerebrospinal Syphilis," Journal of the American Medical Association 69, no. 25 (1917): 2087–9; Carlyle N. Haines, "Salvarsan in Syphilis," Pennsylvania Medical Journal 24 (1921): 839–41.


Derived largely from arsenic, a highly toxic substance, Salvarsan was a frightening remedy. While more effective than mercury, its use was accompanied by a panoply of side effects—from the mild (dermatitis, gastro-intestinal distress) to the severe (ocular damage, cardiac distress, edema). In rare cases, death resulted. In a review of 6,308 syphilis patients admitted between 1922 and 1932, Wenger counted a total of 225 adverse reactions to Salvarsan—including three fatalities from arsenical poisoning.58O.C. Wenger and Lida J. Usilton, "Notes on the Syphilis Clinic, United States Public Health Service, Hot Springs, Arkansas," Journal of Venereal Disease Information 15, no. 6 (1934): 210. It is impossible to verify these morbidity and mortality figures, as the clinic operated free from federal oversight. Because of this, and also because of the clinic's generally poor record-keeping practices, the number of "adverse reactions" may be higher than what Wenger reported. For more on the latter problem, see C.H. Waring to the Surgeon General, January 23, 1923, VD Division Records. It appears that severe reactions to Salvarsan were more common here than elsewhere.59In a 1940 study, clinic personnel revealed that nearly 2.5 patients per thousand experienced "severe reactions" to Salvarsan—a rate higher than the 1.99 per thousand reported by the Cooperative Clinical Group's studies of syphilis. Waugh and Milosivic, "Severe Reactions." Cognizant of the fact that "the duration of anti-syphilitic treatment at the Hot Springs clinic is for a relatively short time," Wenger's staff rushed to experiment with untested modes of therapy. The adoption of an "intensive and continuous plan of treatment" contributed to the clinic's high rate of serious complications.60Wenger and Usilton, "Notes on the Syphilis Clinic," 209. For further evidence of serious medical complications following upon the clinic's intensive plan of syphilis treatment, see George E. Tarkington, "Value of Liver Function Test in Arsenical Therapy," Journal of Venereal Disease Information 7, no. 1 (1926): 24–5. For details of a specific injury, see Paul S. Carley, "Infarction of Buttock from Intra-Muscular Injections of Mercury Benzoate," Journal of Venereal Disease Information 17, no. 10 (1936): 281–3. It bears noting here that during the 1920s and 1930s, the idea of "informed consent" had not become a universally recognized principle within medical ethics. Because of this, scientific investigators were not required to obtain patient permission before proceeding with experiments. Those housed within custodial institutions (public hospitals and clinics, asylums, prisons, orphanages, etc.) were especially targeted for human subjects research, with the justification often being that they owed society a debt in exchange for the free treatment they received. For more on this, see Susan Lederer, Subjected to Science: Human Experimentation in America before the Second World War (Baltimore, MD: Johns Hopkins University Press, 1997).
Such was certainly the case for Forrest LaPrade. A twenty-four-year-old Texan who arrived in Hot Springs in March 1930, LaPrade's original intention was to "boil out nicotine and malaria" through the city's "healing waters." Directed to Wenger's clinic for a physical, LaPrade was found to be syphilitic. Over the next few weeks he received seven shots of Salvarsan and eleven of mercury. His condition then worsened.61For the details of LaPrade's case, see G.L. Collins to the Surgeon General, October 11, 1932, VD Division Records.
On May 2, 1930, LaPrade complained of a "slight oedma" of the face, which his physician noted was "characteristic of arsenical poisoning." By the next day, he displayed a "face intensely swollen," along with a fever and an accelerated heart rate. After being diagnosed with erysipelas, LaPrade was transferred by a friend to a nearby hospital, where for twenty-eight days he experienced "untold agonies." Hoping to heal his swollen face, from which dripped "large drops of yellow corruption," LaPrade's doctors covered him with a white, glue-like paste, a remedy that produced a constant itching sensation that left the Texan "at the point of death." "I was actually skinned alive," LaPrade later said, describing how the itching left him "scaled like a fish." Unable to sleep, LaPrade's condition was so bad that his body "trembled like a leaf and even shook or quivered the bed." "I suffered, cried, and prayed as one who was in the doorway of Hell," he recalled with horror. "But for the Lord, I would have been six feet of earth."62Forrest D. LaPrade to Mr. Wright Patman, June 10, 1930, VD Division Records.
Although few patients faced an ordeal like Forrest LaPrade's, the clinic's experiments failed to produce "new and better methods to fight venereal diseases."63M.J. White, "Next Steps in the Field of VD Control from the Standpoint of the United States Public Health Service," Journal of Venereal Disease Information 7, no. 1 (1926): 173. A report from the PHS's Division of Venereal Diseases spoke in disappointed terms: "It was hoped that this clinic would prove useful from a research standpoint, but because of the transient character of the patients, results thus far have not been up to expectations."64"Meeting of the Advisory Committee to the Division of Venereal Diseases, United States Public Health Service, May 16, 1927," Journal of Venereal Disease Information 8, no. 8 (1927): 303. And as late as 1936, clinic personnel were still reporting on the "comparatively small number of treatments given" to patients—a reference to how few individuals completed a full course of anti-venereal treatment.
Figure 2: Sex Differentials in Syphilis by Stage of Disease upon Arrival in Hot Springs, 1922–1932

Healing the "Other": Women and African Americans at the Hot Springs VD Clinic
Because their attempts to accelerate the curative process largely failed, Wenger's staff also investigated ways of keeping patients within Hot Springs for longer periods of time. This search for extra-medical means of disease control had a racial foundation, one that becomes clear through an examination of doctors' experiences with female patients. Initially, Wenger and his staff harbored quite negative attitudes toward women, who were seen as "uncontrolled spreaders of infection" and a "menace to the community at large."65Wenger, "The Need for Social Hygiene"; Oliver C. Wenger, Annual Report for 1923, Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives. With the passage of time, however, clinic personnel became increasingly sympathetic to the plight of female health-seekers—even those who supported themselves through prostitution while receiving treatment. From these sentiments (which extended only to whites) emerged a non-traditional disease control program, one rooted not only in testing and treatment, but also in socioeconomic measures—including financial aid for food and housing.

Wenger's first few years in Hot Springs were characterized by an intensive crackdown on the city's red-light districts, which had re-opened in the aftermath of World War I. Hoping to prevent local brothels from recovering their former strength, in January 1921 the PHS presented an ultimatum to municipal authorities, explaining that unless the city abolished its regulated district the agency would quarantine all individuals who came to Hot Springs seeking treatment for disease—venereal or otherwise. Recognizing that it would "prove a great financial blow to the city if this patronage were lost," the PHS argued that it was "absolutely inconsistent to permit men to go there for the cure and, at the same time be exposed to reinfection through the agency of an open red-light district." Women too would be subject to these measures, as some of the female patients in Hot Springs were prostitutes who "carry on their profession while under treatment."66"Hot Springs Threatened With Loss of Patronage: Health Resort Must Eliminate Red-light District," The Social Hygiene Bulletin 8, no. 1 (1921): 8.
This seemed clear from a report Wenger received from the Interdepartmental Social Hygiene Department (ISHD) in 1922. A governmental entity tasked with investigating the relationship between prostitution and VD, the ISHD in 1921 sent an agent named Blanche Young to Hot Springs. Upon questioning a few girls "of the prostitute type" found within the city's public dance halls, she concluded that no progress against VD would be forthcoming unless the federal government abolished its system of regulated prostitution. One of the prostitutes Young met with informed her that "she had gone to the city for medical treatment and was under the care of a private physician." On another occasion, Young encountered a "very fast looking girl enter[ing] an automobile occupied by three young men who were obviously under the influence of liquor." "A little later," Young continued,
I saw this automobile stop and the men 'pick up' two girls. This was about 11:43 PM. The men talked to the girls on the street, inducing them to enter the car, immediately driving off. The next day I recognized in both the G.U. [genito-urinary] and syphilis clinics one of the girls who was present in the dance hall.67L. Blance Young to O.C. Wenger, February 8, 1932, Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives.

Reports such as these inclined Wenger toward an all-out assault on the city's red-light district. As during wartime, Hot Springs's response to this federal ultimatum was regretful compliance. The death of the city's physician-mayor J.W. McClendon—"the leader of the wide-open town policy"—eased Washington's task. With the removal of this "obstacle," the PHS convinced local law enforcement officials to fall in line.68O.C. Wenger to David Robinson, April 18, 1921, Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives. By the summer of 1922, five brothels had been shut down; by 1923, their number had been reduced by half.69 Information on brothel closures comes from my own analysis of police dockets from the City of Hot Springs, 1920–1923. These documents can be found in the Garland County Historical Society Archives, Police Department Records, Vertical Files, Garland County Historical Society, Hot Springs, Arkansas. In 1918, before the initial crackdown on prostitution, sex-workers accounted for almost one-fifth of all criminal arrests in the city. These results bore out the federal government's conclusion that local personnel had been "very successful" in "eliminating houses of prostitution" in Hot Springs.70First Deficiency Appropriation Bill, 1921: Hearing before Subcommittee of the House Committee on Appropriations (Washington, D.C.: Government Printing Office, 1921), 568.
This assessment proved premature. The interwar years brought new life to prostitution. While initially complying with the PHS, steep declines in revenue from saloons and bawdy houses prompted municipal officials to change their minds.71"Hard Sledding for Bankrupt City," Yearbook of the City Managers' Association 6 (1920): 85–6. In the late 1920s, the city's mayor "[threw] the town wide open" to prostitution, and in the next decade, cases of "female patients street-walking or soliciting" were "almost of daily occurrence."72Oliver C. Wenger, "The Transient-Indigent-Medical Problem at Hot Springs National Park, Arkansas," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives. The clinic did little to oppose this challenge to federal authority. A 1934 visitor to the city remarked that Hot Springs was "the only national park where gambling, imbibing, and prostitution go unmolested."73Ray Hanley, A Place Apart: A Pictorial History of Hot Springs, Arkansas (Fayetteville: University of Arkansas Press, 2011), 81; "Hot Springs Would Secede," Today 3 (1934): 23.
What explains this reversal? For one, it appears that clinic personnel had little appetite for prolonged conflict with the array of local forces (officials, doctors, and brothel owners) opposed to the abolition of prostitution. More important, however, were the interactions clinic personnel had with female patients—many of whom sold their bodies for sex while seeking VD treatment.
Consider the experience of a "young white woman" from Tennessee named "O.J." Orphaned since childhood, O.J. had grown up at the House of the Good Shepherd in Memphis. With "limited" opportunities, she then supported herself largely through prostitution—by which she contracted both syphilis and gonorrhea. Upon arriving in Hot Springs, O.J. found work as a boarding house maid. Subsequently accused by her landlady of "running around with men," O.J. found herself back on the streets. For the remainder of her stay, she supported herself through prostitution, a decision defended with three words: "I must eat." While concerned over the number of "boy friends" this "more than ordinarily attractive" woman had infected, Wenger sympathized with O.J.'s plight, explaining to his superiors that "she was a good patient and reported regularly for treatment." Summarizing her case, the PHS agent conceded that "it is hard to be chaste and hungry."74Wenger, "The Transient-Indigent-Medical Problem."

Interactions with patients like O.J. had a dramatic impact on clinicians, who came to accept prostitution not as an indication of immorality, but as a consequence of the adverse circumstances many female patients faced.75Wenger, Annual Report for 1923. In one of his earliest reports, Wenger spoke of the "large number of female patients" who arrived in Hot Springs with "no funds" and "no friends." With work "scarce" in the city, many of these women—in a "much discouraged" state—were "forced by dire necessity to support [themselves] by prostitution."76Oliver C. Wenger, "History of United States Public Health Clinic, Hot Springs, Arkansas," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives. The experiences of patients like O.J. were "not unique nor unusual, but exactly what goes on as these transients move across the country in their efforts to receive free medical service."77 "Any person who engages in travel," Wenger maintained, "may be the carrier of a communicable disease." "Every health officer knows," he reminded his superiors, "of instances, when, from one single source, hundreds and thousands of new cases have developed." Oliver C. Wenger, "The Indigent, Transient Problem and Its Relation to Public Health," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives. Criticizing those who argued that prostitution could not be tolerated, Wenger explained that "as social workers and health officers, we must change our own attitude and remember that we ourselves would become transients seeking medical services if they were not available at home. This is only natural."78Ibid. In connection with Wenger's apparent acceptance of prostitution in Hot Springs, it is interesting to note that while overseeing a VD control program in Puerto Rico during the Second World War, the PHS official was privately reprimanded for proposing "methods of registration and identification of prostitutes which seem quite out of line" with the federal government's official policy of repression. For more on this, see Surgeon General Parran to Senior Surgeon O.C. Wenger, March 23, 1942, Thomas Parran Papers, Series 1, Box 5, University of Pittsburgh, Pennsylvania. Hereafter, Parran Papers.
Consistent with his new understanding of prostitution, Wenger's interactions with female patients displayed a lack of moralizing. In lectures on how to "prevent a second infection," he endorsed the use of condoms and taught women "the value of prophylaxis and also contraceptives, or birth control methods." A typical lesson began with a discussion of female anatomy and concluded with demonstrations of birth control techniques.79In educating his patients on the use of contraceptives, Wenger was taking a risk. As he noted in a 1926 letter sent to Thomas Parran (the recently-appointed director of the PHS's Division of Venereal Diseases), "the whole subject of prophylaxis is T.N.T. at this stage of the game," and as such, advocating too forcefully on behalf of birth control measures "might innocently start some unwelcome comment"—particularly in the South. On account of this, Wenger generally advised that the PHS "let the State V.D. men do as they please"—another sign of the impact local forces had on the federal government's efforts. For more, see Oliver C. Wenger to Thomas Parran, October 23, 1926, Parran Papers. While initially concerned about how female patients would react to these frank methods, Wenger reported that "there has been no embarrassment on the part of the volunteer subjects or the patients looking on. The remarks and questions asked during the demonstrations are amazing."80O.C. Wenger to Dr. White, January 13, 1925, VD Division Records.
The clinic's female patients also encouraged Wenger to search for economic solutions to the country's VD epidemic. Consider the 1933 case of "Mrs. W." A white, college-educated woman who "came here all the way from old Mexico" after having been deserted by her husband (who infected her with syphilis) and having "suffered losses in the general depression." Upon arriving in Hot Springs, Mrs. W. initially stayed with a "colored friend." When this woman's relatives moved in, Mrs. W. informed clinic personnel that she was "planning to 'hitchhike' her way back to Nogales, Arizona," where friends would take her home. Believing such a trip would be "practically impossible," Wenger turned to local welfare agencies, "who agreed to pay half of her fare." The remainder was "made up by clinic personnel." Discussing her case in a report to his superiors, Wenger noted that "this is just another instance, in which, if maintenance could have been arranged for a longer period of time, the patient could have probably improved sufficiently to take her place again among her friends and be self-supporting."81Wenger, "The Transient-Indigent-Medical Problem."
Like O.J. and Mrs. W., most of the women who made their way to the Hot Springs clinic in the 1930s were white.82During the clinic's formative years, white women never accounted for more than one-fifth of the clinic's annual caseload. Between 1928 and 1936, however, their numbers steadily grew, reaching a peak of 2,353 in 1935—a year in which they represented nearly one-third of all patients treated. During the same period, African Americans' share of the clinic's annual caseload declined from 36.9 percent to 20.3 percent—a trend especially evident among females. O.C. Wenger, "Summary Statistical Data," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives. They received a much more sympathetic response than did the city's black health-seekers. Consider the case of Charley Wade Bradshaw. Shortly after entering the clinic on September 3, 1927, Bradshaw—a twenty-five year old black man employed as a porter by the Oklahoma City Railway Power House—was diagnosed with neurosyphilis and placed on a regimen of mercury. For six weeks, Bradshaw's savings enabled him to rent a room at a colored hotel, but on October 19, he was reported "AWOL." One year later, an Oklahoma City law firm supplied the reason for this abrupt departure. Coming to Hot Springs after company doctors "advised him that he had bad blood," Bradshaw left after running out of money for room and board. As an attorney informed Wenger, Bradshaw was "in a bad condition physically," and because he had "no means whatever," anyone who tried to help him "will have to do so at their expense."83Walter Martin to O.C. Wenger, March 2, 1928, VD Division Records.
Wenger apparently made no effort to pay for Bradshaw's expenses, despite his recognition of the socioeconomic inequalities that imperiled black health.84Between 1922 and 1932, the number of African American visitors listed in the "unskilled labor" category was "nearly twice as high" as the comparable figure for whites. O.C. Wenger, "An Analysis of 10,000 Cases of Syphilis," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives. While concurring that venereal diseases were "playing havoc within the Negro population of the country," he criticized those who interpreted these findings as evidence of African Americans' "absolute lack of morality." The observed differential between whites and blacks, commented Wenger, "does not mean that there is a considerable difference in the morals of these different groups." The critical variable was African Americans' "social economic status"—in particular, their "more limited" educational and employment opportunities. "When the social and economic backgrounds of the two races are considered," he concluded, "there seems to be little difference in the incidence of infection."85Oliver C. Wenger, "Analysis of 10,000 Cases of Syphilis," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives.

Improving black health-seekers' access to treatment required more than a rejection of the "syphilis-soaked negro" stereotype. When it came to removing institutional and economic barriers confronting African American VD patients, Wenger did little. He refused to challenge Hot Springs's adherence to Jim Crow, which confined African Americans to an "exterior observation" of all but two of the city's bathhouses. In addition to the "great disadvantage" they faced due to the "lack of proper accommodations in hotels and bathhouses," black patrons had fewer opportunities for securing therapeutic services than did whites. The Depression felled the one institution—the Woodmen of the Union Hospital—specifically catering to blacks.86 A.W. Hunton, "The American Carlsbad," The Voice of the Negro 3, no. 5 (1906–7): 331; C. Melnotte Wade, "Hot Springs—Its People," Colored American Magazine 10, no. 1 (1906): xviii; O.C. Wenger, "The United States Public Health Service Clinic at Hot Springs National Park, Arkansas," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives; O.C. Wenger to Surgeon General, July 27, 1934, VD Division Records.
Black patients also faced the racial hostility of local physicians—some of whom worked in the PHS clinic. Believing that their higher rates of syphilis and gonorrhea stemmed from "the negro's almost absolute lack of morality and cleanliness," the resort's white doctors contended that southern blacks were "little better than animals with strong sexual passions."87 Thompson, Syphilis, 52. Some believed that emancipation constituted the primary cause of syphilis's spread "among the negro population of the South," as rampant promiscuity created a situation in which "the very existence of the race is threatened."88L.R. Ellis, "Address of the Chairman of the Section on Dermatology and Syphilology," Journal of the Arkansas Medical Society 6 (1909): 44; Loyd Thompson and Lyle B. Kingerly, "Syphilis in the Negro," American Journal of Syphilis 3 (1919): 396.
Racist attitudes were on display within the Hot Springs VD clinic. Admitted in July 1925, George Smith was a black man who came to the attention of local authorities after his arrest for "night prowling." While a judge ordered his release on the condition that he leave town, a Wassermann test revealed that Smith was infected with syphilis. Shortly after Wenger prevailed upon the city to permit his entrance into the PHS facility, trouble began. One day while receiving an injection of mercury, Smith reportedly became "impudent," and the doctor treating him "lost his temper and threatened to ruin" the man. Upon hearing of the incident, Wenger informed Smith to "remain away" from the clinic until the physician in question—a Dr. Abington—left. Though not expelling him, Wenger warned the doctor not to "cuss" the patients, and in his review of the case, the PHS official observed that Abington "was born and raised in the South, and [was] prejudiced toward all aggressive negroes."89O.C. Wenger to the Surgeon General, July 20, 1925, VD Division Records .
With the advent of the Great Depression, fewer and fewer men such as Charley Bradshaw and George Smith entered the Hot Springs clinic. As the economic misery of the 1930s increased, the proportion of black men and women admitted to the clinic declined precipitously; whereas in the 1920s, roughly one-third of the city's health-seekers were African American, by the middle part of the 1930s, this figure had fallen to about one-fifth. Those able to pay for a stay came later in the course of their infections than did whites, and in addition to presenting less curable forms of illness, they left Wenger's clinic much earlier than did white men and women.90On average, between 1922 and 1936, African American rates for tertiary syphilis were ten percentage points higher than those of their white counterparts, who also presented 8 percent more primary and secondary cases than did black syphilitics. O.C. Wenger, "Classification of Syphilis Cases, U.S. Public Health Service Clinic," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives. A 1940 study revealed that the average white syphilitic received twelve shots of Salvarsan, and blacks only nine.91Waugh and Milovich, "Severe Reactions," 390. For further evidence of the unfavorable therapeutic outcomes for black patients, see J.R. Waugh and W. Burns Jones, "Genito-Urinary Survey of 1,625 Male Patients, United States Public Health Service Venereal Disease Clinic, Hot Springs, Ark.," Journal of Venereal Disease Information 13, no. 1 (1932): 9.
Instances of racial discrimination continued. In 1941, a PHS officer reportedly entered a number of "reputable Negro business places" in nearby Texarkana, arresting several "young ladies," and then transporting them to Hot Springs for treatment—all without testing them for venereal disease.92"Officer Uses 'Gestapo' Methods: Texarkanians Terrorized, Business Houses Molested," Arkansas State Press, July 25, 1941, 1. Such tactics soured many black syphilitics on Hot Springs.93For likely racial discrimination, see Paul Carley, "Infection with Syphilis Masked by Gonorrhea," Journal of Venereal Disease Information 18, no. 2 (1937): 21–4. For their part, black newspapers discouraged readers from journeying into central Arkansas, noting that northern health resorts and spas were "more attractive than Hot Springs" on account of the latter's "awful...Jim Crow cars and other uncivilized offerings to the colored visitor."94"Negroes Can Bathe at French Lick Springs," The Michigan State News, Tuskegee Institute News Clippings File.
Clinic to Camp
From the beginning, clinic personnel were wary of attracting local citizens' ire. Hot Springs's patients frequently "[ran] into trouble with the police for housebreaking and robbing. " Local residents resoundingly objected to "the presence of such large numbers of indigent VD cases on the city streets."95"Hot Springs Judge Wroth over 'Dumping' of Indigent Diseased Transients in City," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives; Wenger, "The Transient-Indigent-Medical Problem"; O.C. Wenger to Surgeon General, July 27, 1934, VD Division Records. As early as the mid-1920s, Wenger called on the federal government to provide "some means of housing these indigent patients, or at least of providing them with sufficient food while they are under our care."96O.C. Wenger, "United States Conducts Clinic for Venereal Diseases," 103. Such aid never came.
During the Depression—as the city was "swamped with applicants seeking medical aid"—"begging, borrowing, and stealing" intensified.97Oliver C. Wenger to Taliaferro Clark, August 29, 1931, NPS Archives. Many of these applicants, wrote Wagner, belonged to a "much higher type group," individuals who in normal times would not have had to avail themselves of free, government-provided services.98O.C. Wenger, "The Transient-Indigent-Medical Program," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives. Aware of the ways his clinic was "causing objection and criticism from certain groups of citizens," in 1933 Wenger again asked for federal housing of indigent patients. His next budget included monies courtesy of the Arkansas Transient Bureau (ATB), a branch of the Federal Transient Bureau, to provide "free room and board" at "$1.00 per day per patient," as well as funds for hospitalization, telegrams, minor emergencies, and transportation home.99Ibid.
During its first month in operation, the ATB provided shelter, clothing, food, and medical attention to over 2,300 VD patients—black as well as white, female as well as male. The program reaped immediate dividends: according to state officials, only one year after implementing Wenger's "maintenance" plans, the number of venereal health-seekers leaving Hot Springs non-infectious increased by 38 percent.100R.O. Brunk, "Some Interesting Facts," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives. Echoing these sentiments, in January 1934, Wenger wired Washington praising the ATB for "giving out free room and board," noting that as a result of this "most of the old patients are remaining because they are getting free room and board and are taking more treatment."101Oliver C. Wenger to Dr. Vonderlehr, January 10, 1934, NPS Archives.
Figure 3: Salvarsan Injections Per Patient, 1922–1936

As diseased men and women descended onto Hot Springs, by early 1935 the ATB was providing for 4,000 diseased indigents.102McCully, "The United States Public Health Service." City officials claimed that many patients were "irresponsible as to their personal conduct"; every day, one local paper reported, twenty-five health-seekers faced arrest on charges of drunkenness and disturbing the peace.103Brunk, "Some Interesting Facts," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives; "Hot Springs Judge Wroth over 'Dumping' of Indigent Diseased Transients in City," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives. "If the federal government continues to invite the scum of the earth here," complained a judge to the PHS, "I guess we'll just have to move out and give the town to you."104"Hot Springs Judge," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives.
Hot Springs officials began resisting calls for assistance, even refusing to admit dozens of children whose parents were receiving treatment into the public school system. Despite Wenger's "most vehement protests," and despite repeated assurances that it was "perfectly safe" for these children to mingle with local children, municipal leaders were adamant.105Oliver C. Wenger, "A Plan for the Consolidation of all Medical Measures for Transient Relief in Hot Springs, Arkansas," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives. They began to push for the removal of the clinic's "undesirable" indigent transients.106"Council Approves New Transient Plan," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives.
Conceding that patients "cannot be left to roam at will and get into difficulties on the streets of Hot Springs," federal officials and the ATB considered construction of a camp on the city outskirts to house clinic patients and "give them wholesome occupation and recreation."107Antoinette Cannon, "Hot Springs Transient Program," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives. Initially, Wenger opposed these plans, but in order to "meet the needs of patients and the community," in 1934 the ATB began building a camp "for lone men who are under care in the United States Public Health Service clinic.108Ibid.

A year later, Camp Garraday opened on a thirty-three acre tract with a sixty-bed infirmary, nine barracks, kitchen, dining hall, and recreation building. During its first year, the ATB facility quartered five hundred white male transients.109O.C. Wenger, "A Plan for the Consolidation of all Medical Measures for Transient Relief in Hot Springs, Arkansas," September 5, 1935, NPS Archives. While these men—whom Wenger labeled the clinic's "hardest problem"—benefited from the "good food," shelter, immediate medical attention, and recreational opportunities provided directly by the federal government, white women and African Americans of both sexes continued to subsist under the old plan, by which they were "maintained in rooming and boarding houses throughout the city."110O.C. Wenger, "The United States Public Health Service Clinic at Hot Springs National Park, Arkansas," Oliver C. Wenger Papers, Box 1, University of Arkansas for Medical Sciences Archives.
Camp Garraday embodied the PHS's eugenic understanding of VD. While Wenger labeled white male patients a "problem," they were central to his ideology of "race conservation" and thereby worthy of privileges. Other patients might receive very modest financial aid, but they had to find sources of food and shelter, and felt the full force of the city's loathing. By contrast, white male patients received care on site, in a domiciliary setting. And Wenger sought to expand the camp's capabilities. In his 1936 budget, he recommended $55,320 for additional forms of support—including a butcher, a recreational supervisor, a housing director, a nursery, and a children's school (with principle and one teacher)—for Camp Garraday's residents.111Oliver C. Wenger, "A Plan for the Consolidation of All Medical Measures for Transient Relief in Hot Springs, Arkansas" (September 5, 1935), NPS Archives.
Wenger's plans never came to fruition. Local white citizens quickly and vehemently complained that Camp Garraday, "a Frankenstein monster," restored the "old stigma that Hot Springs is a place only for the treatment of venereal diseases." As the director of the Hot Springs Reservation explained, the PHS's efforts threatened to "ruin the results of the past hundred years of our history, to say nothing of the millions of dollars invested in the resort by private capital." The existence of Camp Garraday functioned to "make the place undesirable for pay patients."112As one local authority put it, developments of the early 1930s had given the health resort's more wealthy visitors the impression that "the transients being treated here were so numerous that [they] would overrun everything," and on account of this, the city had become "undesirable for pay patients." Thomas J. Allen to Arno B. Cammerer, July 23, 1934, NPS Archives.

Unable to overcome residents' objections to Wenger's maintenance program and the ATB's camp plan, the federal government terminated the Transient Bureau in 1936 and Camp Garraday ceased to house patients. Venereal health-seekers wishing treatment in Hot Springs were required to bring "sufficient funds available to pay their room and board over a period of at least ninety days."113John J. McShane to All Local Health Authorities, March 10, 1936, VD Division Records. For Oliver Wenger, who left Hot Springs in 1937 to take part in Chicago's Syphilis Control Program, it was a bitter ending. It appeared to him that Hot Springs was in no better shape than when he first arrived fifteen years earlier.
The same year Wenger left Hot Springs, Congress passed the National Venereal Disease Control Act. Allotting funds to the states, this legislation enabled a dramatic expansion in the nation's anti-venereal infrastructure. Arkansas soon felt the act's effects: prior to 1937 there were no state-run VD clinics here; by 1943, there were eighty-three. These new medical facilities treated fifteen thousand patients per year, far exceeding the heyday of the Hot Springs VD clinic.114"Venereal Disease Control," Arkansas Health Bulletin 1, no. 3 (1944): 6–9. In tandem with the mass production of penicillin in the 1940s, these developments led to a precipitous decline in the nationwide incidence of syphilis and gonorrhea. By the early 1950s, the country's VD "epidemic" had ended, and although rates for both syphilis and gonorrhea rose in subsequent decades, the government's model VD clinic would play no part in post-war developments.
Conclusion: Race, Hot Springs, and Tuskegee
The history of the Hot Springs VD clinic reveals how eugenics shaped the federal government's response to syphilis and gonorrhea. The facility's day-to-day operations show how the goal of "race conservation" structured patient experiences and outcomes. On account of the high volume of white syphilitics seeking admittance, clinic personnel became increasingly sympathetic to patients' circumstances and needs, and eventually, this sympathy manifested itself in a medical program that included free treatments as well as stipends for housing and food. While patients, regardless of race or sex, benefited from these extra-medical measures, it is unlikely the PHS would have launched such an approach to VD had not the primary beneficiaries been white males. The Camp Garraday transient center doled out special services to clinic patients because they were white men.

How did eugenics and scientific racism unfold at Hot Springs as compared with Tuskegee? As the failure of its venereological research program suggests, Hot Springs is a story about subjects becoming patients. In Tuskegee, the opposite occurred. What began as a series of mass treatment campaigns ended up as a horrific forty-year research program revolving around the denial of medical services. Tuskegee's creators tried to explain their complicity by invoking the Great Depression, claiming that their actions resulted from agency budget cuts that rendered additional funding for VD treatment impractical. However, just as the Depression deepened its hold, the PHS began pouring money into the Hot Springs clinic, whose patients were provided with drugs as well as with funds for food and shelter. The clientele at Wenger's clinic were primarily white; those enrolled in the Tuskegee study were black.
Race played a determining role in the PHS's attack on syphilis and gonorrhea. In broadening the scope of historical study beyond Tuskegee, and in particular by looking at the agency's policies toward white patients, the extent of the government's racialized response to VD becomes clearer.
About the Author
Elliott Bowen is a professor of history at Nazarbayev University and a historian of medicine and public health in the modern United States. His research explores the history of sexually transmitted diseases. Bowen is currently working on a book-length project about the history of Hot Springs, Arkansas.
]]>